Shi Houyin, Ou Yunsheng, Jiang Dianming, Quan Zhengxue, Zhao Zenghui, Zhu Yong
Department of Orthopaedics, the First Affiliated Hospital of Chongqing Medical University, Chongqing, China.
Medicine (Baltimore). 2017 Jan;96(1):e5718. doi: 10.1097/MD.0000000000005718.
A prospective, randomized, double-blind, placebo-controlled study was performed. The routine usage of TA in spinal surgery is controversial. Only a few studies have focused on patients undergoing posterior lumbar surgery for stenosis or spondylolisthesis, although a large clinical cohort exists in the population. This study aimed to evaluate the effect and safety of TA in reducing perioperative blood loss in posterior lumbar surgery for stenosis or spondylolisthesis.
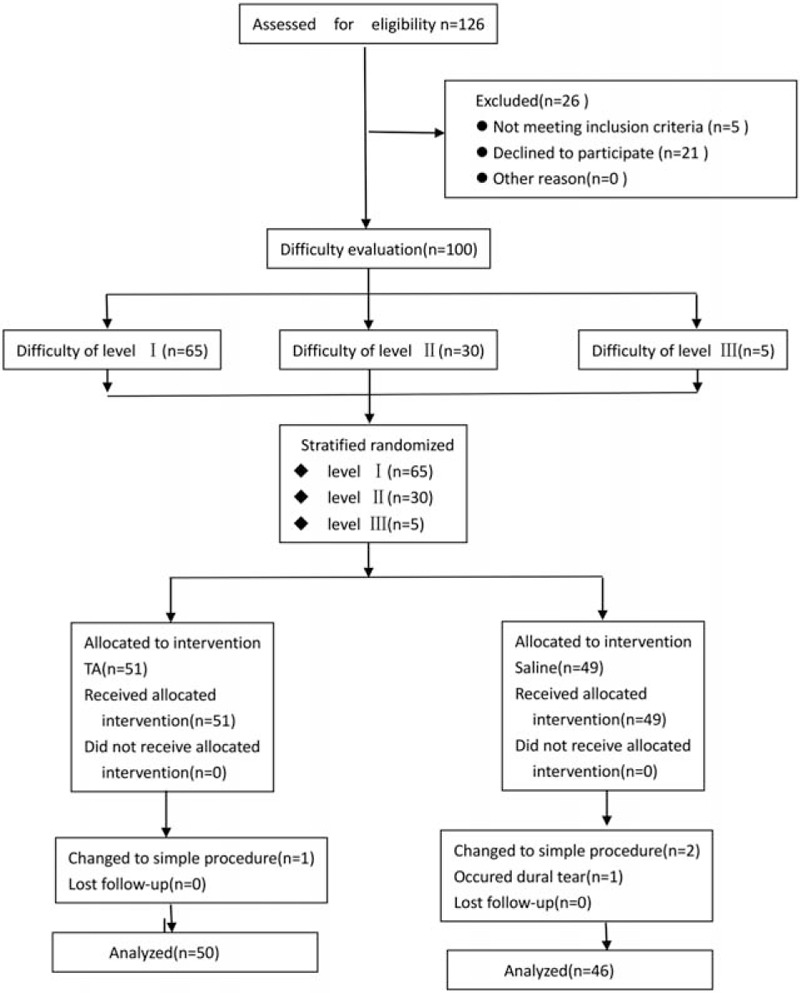
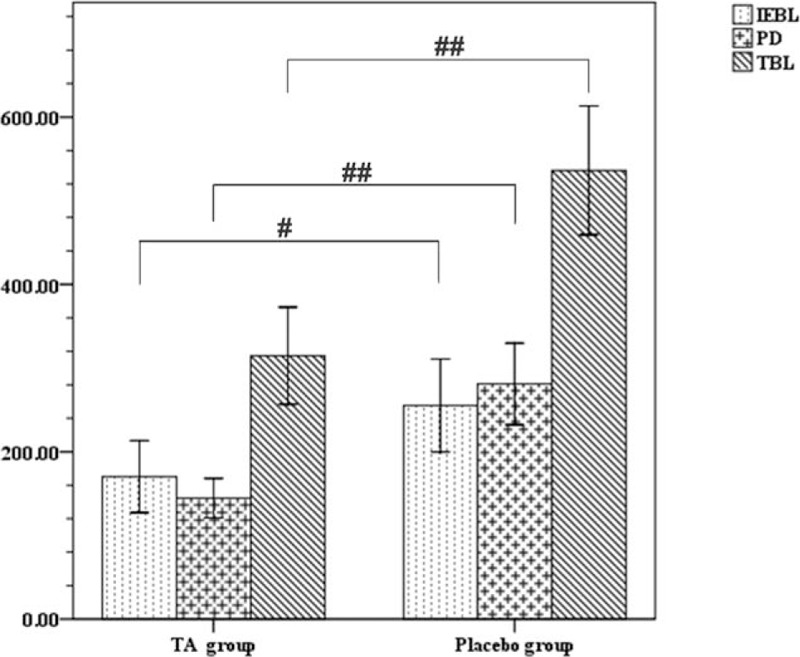
100 eligible patients out of 126 were randomized to receive either a bolus dose of 30 mg/kg TA i.v, a maintenance dosage of 2 mg/kg/h TA, or an equivalent volume of normal saline. The pedicle screw system was used for fixing in all the patients, followed by decompression and posterior lumbar interbody fusion. The primary outcomes were intraoperative estimated blood loss and total blood loss. The secondary outcomes were receiving packed red blood cells and postoperative hemoglobin and hematocrit levels.
In total, 4 patients were excluded from the analyses, 50 patients were in the TA group, and 46 in the placebo group. The demographic and baseline data between the groups were not statistically different. The intraoperative estimated blood loss and the total blood loss were 33% and 41% lower in the TA group than the placebo group, respectively. The blood transfusion rate did not vary significantly (P = 0.191). Except a patient with a dural tear in the placebo group, no other complications were observed.
TA significantly reduced the perioperative blood loss in patients undergoing posterior lumbar surgery for stenosis or spondylolisthesis.
开展了一项前瞻性、随机、双盲、安慰剂对照研究。脊柱手术中TA的常规使用存在争议。尽管该人群中有大量临床队列,但仅有少数研究关注接受后路腰椎狭窄或椎体滑脱手术的患者。本研究旨在评估TA在减少后路腰椎狭窄或椎体滑脱手术围手术期失血方面的效果和安全性。
126例符合条件的患者中,100例被随机分为三组,分别静脉注射30mg/kg的TA推注剂量、2mg/kg/h的TA维持剂量或等量生理盐水。所有患者均使用椎弓根螺钉系统进行固定,随后进行减压和后路腰椎椎间融合术。主要结局指标为术中估计失血量和总失血量。次要结局指标为接受浓缩红细胞输注情况以及术后血红蛋白和血细胞比容水平。
总共4例患者被排除在分析之外,TA组有50例患者,安慰剂组有46例患者。两组间的人口统计学和基线数据无统计学差异。TA组的术中估计失血量和总失血量分别比安慰剂组低33%和41%。输血率无显著差异(P = 0.191)。除安慰剂组有1例患者出现硬脊膜撕裂外,未观察到其他并发症。
TA显著减少了接受后路腰椎狭窄或椎体滑脱手术患者的围手术期失血量。