Horala Agnieszka, Swiatly Agata, Matysiak Jan, Banach Paulina, Nowak-Markwitz Ewa, Kokot Zenon J
Gynecologic Oncology Department, Poznan University of Medical Sciences, Polna 33, 60-535 Poznań, Poland.
Department of Inorganic and Analytical Chemistry, Poznan University of Medical Sciences, Grunwaldzka 6, 60-780 Poznań, Poland.
Int J Mol Sci. 2017 Jan 10;18(1):123. doi: 10.3390/ijms18010123.
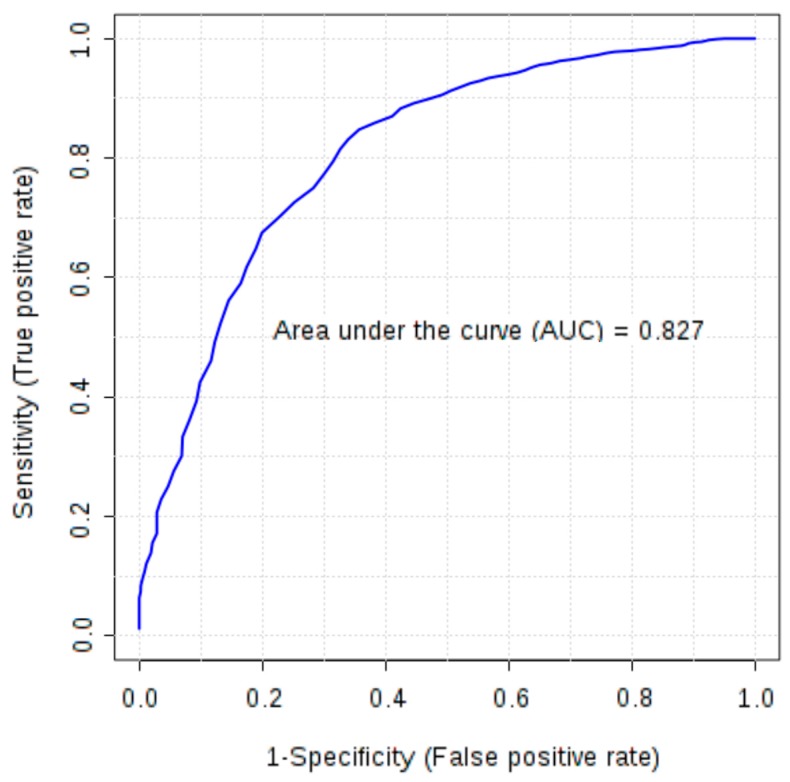
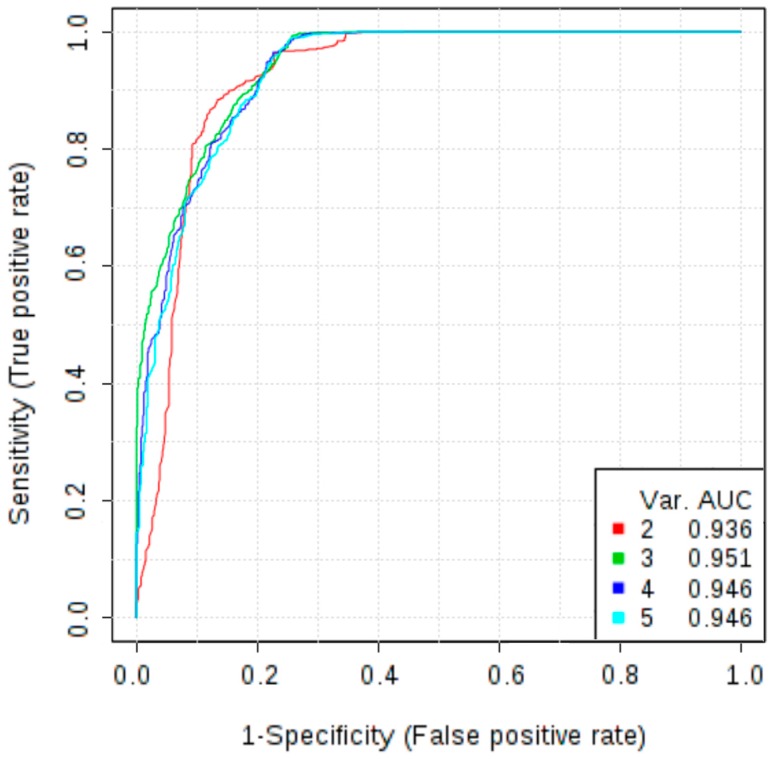
As cancer development involves pathological vessel formation, 16 angiogenesis markers were evaluated as potential ovarian cancer (OC) biomarkers. Blood samples collected from 172 patients were divided based on histopathological result: OC ( = 38), borderline ovarian tumours ( = 6), non-malignant ovarian tumours ( = 62), healthy controls ( = 50) and 16 patients were excluded. Sixteen angiogenesis markers were measured using BioPlex Pro Human Cancer Biomarker Panel 1 immunoassay. Additionally, concentrations of cancer antigen 125 (CA125) and human epididymis protein 4 (HE4) were measured in patients with adnexal masses using electrochemiluminescence immunoassay. In the comparison between OC vs. non-OC, osteopontin achieved the highest area under the curve (AUC) of 0.79 (sensitivity 69%, specificity 78%). Multimarker models based on four to six markers (basic fibroblast growth factor-FGF-basic, follistatin, hepatocyte growth factor-HGF, osteopontin, platelet-derived growth factor AB/BB-PDGF-AB/BB, leptin) demonstrated higher discriminatory ability (AUC 0.80-0.81) than a single marker (AUC 0.79). When comparing OC with benign ovarian tumours, six markers had statistically different expression (osteopontin, leptin, follistatin, PDGF-AB/BB, HGF, FGF-basic). Osteopontin was the best single angiogenesis marker (AUC 0.825, sensitivity 72%, specificity 82%). A three-marker panel consisting of osteopontin, CA125 and HE4 better discriminated the groups (AUC 0.958) than HE4 or CA125 alone (AUC 0.941 and 0.932, respectively). Osteopontin should be further investigated as a potential biomarker in OC screening and differential diagnosis of ovarian tumours. Adding osteopontin to a panel of already used biomarkers (CA125 and HE4) significantly improves differential diagnosis between malignant and benign ovarian tumours.
由于癌症发展涉及病理性血管形成,对16种血管生成标志物作为潜在的卵巢癌(OC)生物标志物进行了评估。根据组织病理学结果,将从172例患者采集的血样进行分组:OC组(n = 38)、交界性卵巢肿瘤组(n = 6)、非恶性卵巢肿瘤组(n = 62)、健康对照组(n = 50),排除16例患者。使用BioPlex Pro人癌症生物标志物检测板1免疫测定法测量16种血管生成标志物。此外,使用电化学发光免疫测定法测量附件包块患者的癌抗原125(CA125)和人附睾蛋白4(HE4)的浓度。在OC组与非OC组的比较中,骨桥蛋白的曲线下面积(AUC)最高,为0.79(敏感性69%,特异性78%)。基于四至六种标志物(碱性成纤维细胞生长因子 - FGF - 碱性、卵泡抑素、肝细胞生长因子 - HGF、骨桥蛋白、血小板衍生生长因子AB/BB - PDGF - AB/BB、瘦素)的多标志物模型显示出比单一标志物(AUC 0.79)更高的鉴别能力(AUC 0.80 - 0.81)。当比较OC组与良性卵巢肿瘤组时,六种标志物具有统计学上的不同表达(骨桥蛋白、瘦素、卵泡抑素、PDGF - AB/BB、HGF、FGF - 碱性)。骨桥蛋白是最佳的单一血管生成标志物(AUC 0.825,敏感性72%,特异性82%)。由骨桥蛋白、CA125和HE4组成的三标志物检测板比单独的HE4或CA125(分别为AUC 0.941和0.932)能更好地区分各组(AUC 0.958)。骨桥蛋白应作为OC筛查和卵巢肿瘤鉴别诊断的潜在生物标志物进行进一步研究。将骨桥蛋白添加到已使用的生物标志物(CA125和HE4)检测板中可显著改善恶性和良性卵巢肿瘤之间的鉴别诊断。