Jing Chu-Yu, Fu Yi-Peng, Shen Hu-Jia, Zheng Su-Su, Lin Jia-Jia, Yi Yong, Huang Jin-Long, Xu Xin, Zhang Juan, Zhou Jian, Fan Jia, Ren Zheng-Gang, Qiu Shuang-Jian, Zhang Bo-Heng
The Liver Cancer Institute, Zhongshan Hospital and Shanghai Medical School, Fudan University, Key Laboratory for Carcinogenesis and Cancer Invasion, The Chinese Ministry of Education, Shanghai, P.R. China.
Oncotarget. 2017 Feb 21;8(8):13293-13303. doi: 10.18632/oncotarget.14530.
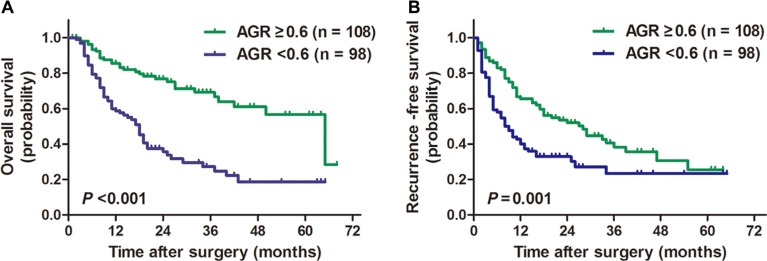
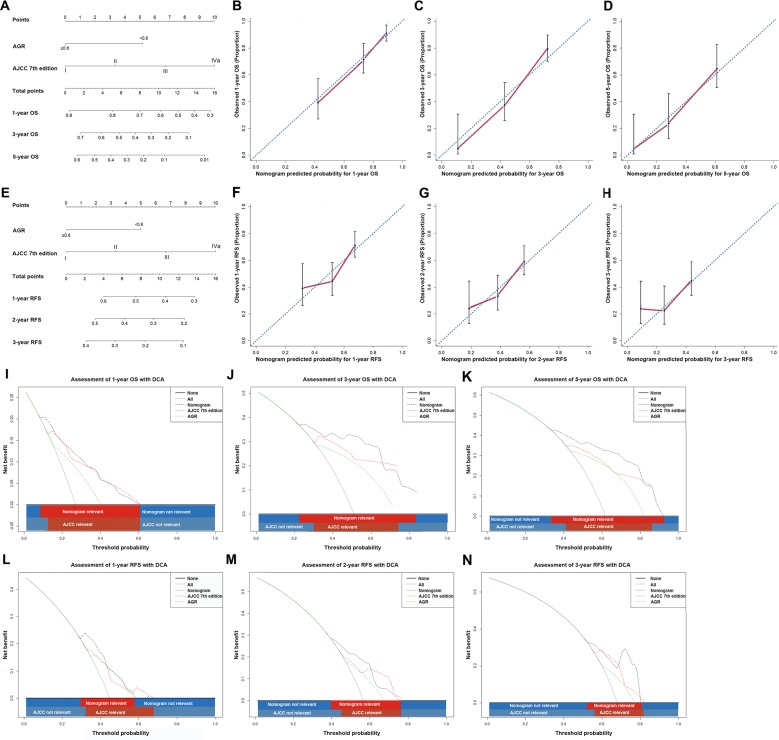
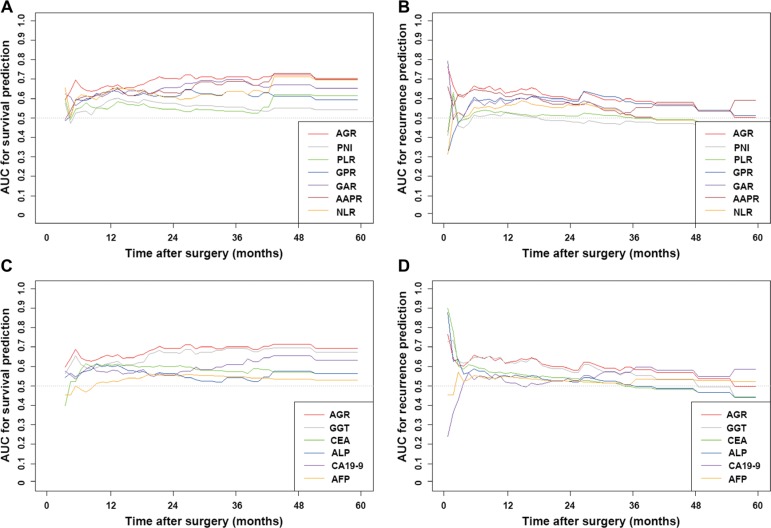
The prognosis of intrahepatic cholangiocarcinoma (ICC) remains poor whereas predictive models for survival prediction in ICC patients following curative resection are limited. Herein, we established a novel inflammation-based score derived from preoperative albumin to gamma-glutamyltransferase ratio (AGR) and evaluated its prognostic significance in ICC patients underwent curative resection. Prognostic value of AGR was retrospectively studied in a cohort comprising 206 ICC patients following curative resection. The predictive performance of AGR was compared with other inflammation-based scores and serological tumor markers in terms of concordance index (C-index). Further, prognostic nomograms incorporating AGR into the tumor-node-metastasis (TNM) staging systems were established to achieve a better discriminatory ability. The optimal cut-off value of AGR was 0.6. Multivariate analysis showed that AGR was an independent predictor for overall survival (OS; P = 0.003) and recurrence-free survival (RFS; P = 0.046). The C-index of AGR was superior to other inflammation-based scores and serological tumor markers in OS and RFS prediction. The established nomograms showed improved predictive accuracy compared with the TNM staging systems alone. These results indicate that AGR is an independent prognostic indicator for ICC underwent curative resection. The incorporation of AGR into the existing TNM staging systems achieved improved predictive accuracy.
肝内胆管癌(ICC)的预后仍然很差,而用于预测根治性切除术后ICC患者生存情况的预测模型却很有限。在此,我们建立了一种基于术前白蛋白与γ-谷氨酰转移酶比值(AGR)的新型炎症评分,并评估了其在接受根治性切除的ICC患者中的预后意义。对一个包含206例接受根治性切除的ICC患者的队列进行回顾性研究,分析AGR的预后价值。将AGR的预测性能与其他基于炎症的评分和血清学肿瘤标志物在一致性指数(C指数)方面进行比较。此外,建立了将AGR纳入肿瘤-淋巴结-转移(TNM)分期系统的预后列线图,以获得更好的鉴别能力。AGR的最佳临界值为0.6。多因素分析表明,AGR是总生存期(OS;P = 0.003)和无复发生存期(RFS;P = 0.046)的独立预测因素。在OS和RFS预测方面,AGR的C指数优于其他基于炎症的评分和血清学肿瘤标志物。与单独的TNM分期系统相比,所建立的列线图显示出更高的预测准确性。这些结果表明,AGR是接受根治性切除的ICC的独立预后指标。将AGR纳入现有的TNM分期系统可提高预测准确性。