Reuken Philipp A, Torres Dorian, Baier Michael, Löffler Bettina, Lübbert Christoph, Lippmann Norman, Stallmach Andreas, Bruns Tony
Department of Internal Medicine IV (Gastroenterology, Hepatology, and Infectious Diseases), Jena University Hospital, Jena, Germany.
Division of Infectious Diseases and Tropical Medicine, Department of Gastroenterology and Rheumatology, Leipzig University Hospital, Leipzig, Germany.
PLoS One. 2017 Jan 11;12(1):e0169900. doi: 10.1371/journal.pone.0169900. eCollection 2017.
Acute cholangitis (AC) requires the immediate initiation of antibiotic therapy in addition to treatment for biliary obstruction. Against a background of an increasing prevalence of multi-drug resistant (MDR) bacteria, the risk factors for the failure of empiric therapy must be defined.
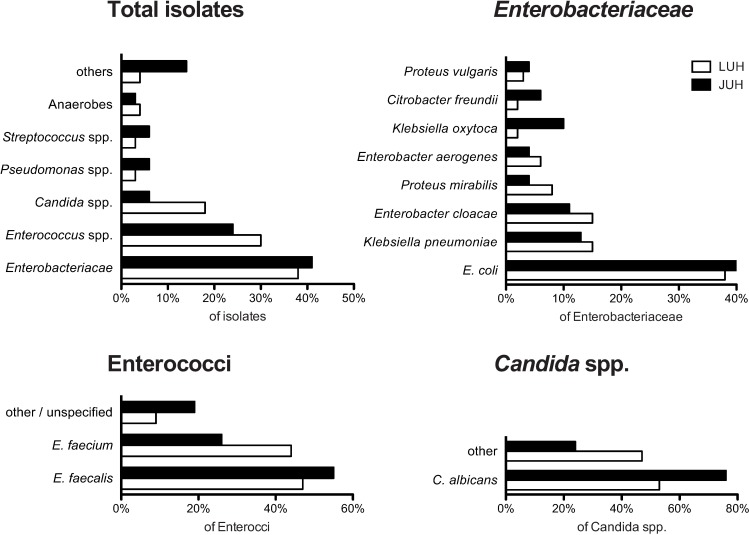
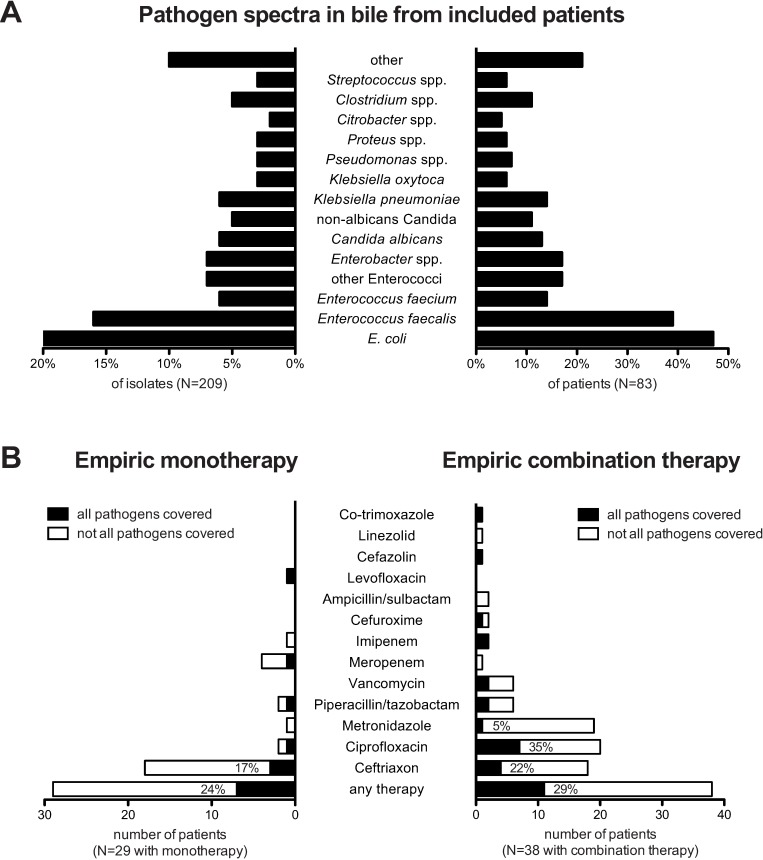
Using a pathogen-based approach, 1764 isolates from positive bile duct cultures were retrospectively analyzed to characterize the respective pathogen spectra in two German tertiary centers. Using a patient-based approach, the clinical and laboratory data for 83 patients with AC were assessed to identify risk factors for AC with pathogens resistant to the applied empiric therapy.
Bile cultures were predominantly polymicrobial, and empiric antibiotic therapies did not cover the full biliary pathogen spectrum in 78% of cases. MDR bacteria were isolated from the bile of 24/83 (29%) patients. The univariate risk factors for biliary MDR bacteria were male sex, nosocomial AC, prior antibiotic exposure and prior biliary stenting, of which biliary stenting was the only independent risk factor according to multivariate analysis (OR = 3.8; 95% CI 1.3-11.0, P = 0.013). Although there were no significant differences in survival or hospital stay in AC patients with and without detected biliary MDR pathogens, the former more often had a concomitant bloodstream infection (58% vs. 24%; P = 0.019), including those involving MDR pathogens or fungi (21% vs. 2%; P = 0.007).
Patients with biliary stents who develop AC should receive empiric therapy covering enterococci and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. These patients are at an increased risk for bloodstream infections by MDR pathogens or fungi.
急性胆管炎(AC)除了要对胆道梗阻进行治疗外,还需要立即开始抗生素治疗。在多重耐药(MDR)菌患病率不断上升的背景下,必须明确经验性治疗失败的危险因素。
采用基于病原体的方法,对德国两个三级中心1764株来自胆管培养阳性的分离株进行回顾性分析,以明确各自的病原体谱。采用基于患者的方法,评估83例AC患者的临床和实验室数据,以确定AC患者中对所应用的经验性治疗耐药的病原体的危险因素。
胆汁培养主要为多微生物感染,78%的病例中经验性抗生素治疗未能覆盖全部胆道病原体谱。24/83(29%)例患者的胆汁中分离出MDR菌。胆道MDR菌的单因素危险因素为男性、医院获得性AC、既往抗生素暴露和既往胆道支架置入,其中根据多因素分析,胆道支架置入是唯一的独立危险因素(OR = 3.8;95%CI 1.3 - 11.
0,P = 0.013)。虽然检测到和未检测到胆道MDR病原体的AC患者在生存率或住院时间上无显著差异,但前者更常伴有血流感染(58%对24%;P = 0.019),包括那些涉及MDR病原体或真菌的感染(21%对2%;P = 0.007)。
发生AC的胆道支架置入患者应接受覆盖肠球菌和产超广谱β-内酰胺酶(ESBL)肠杆菌科细菌的经验性治疗。这些患者发生MDR病原体或真菌感染导致血流感染的风险增加。