Coorey Genevieve M, Neubeck Lis, Usherwood Timothy, Peiris David, Parker Sharon, Lau Annie Y S, Chow Clara, Panaretto Kathryn, Harris Mark, Zwar Nicholas, Redfern Julie
The George Institute for Global Health, Sydney, New South Wales, Australia.
Sydney Medical School, University of Sydney, Sydney, New South Wales, Australia.
BMJ Open. 2017 Jan 11;7(1):e014353. doi: 10.1136/bmjopen-2016-014353.
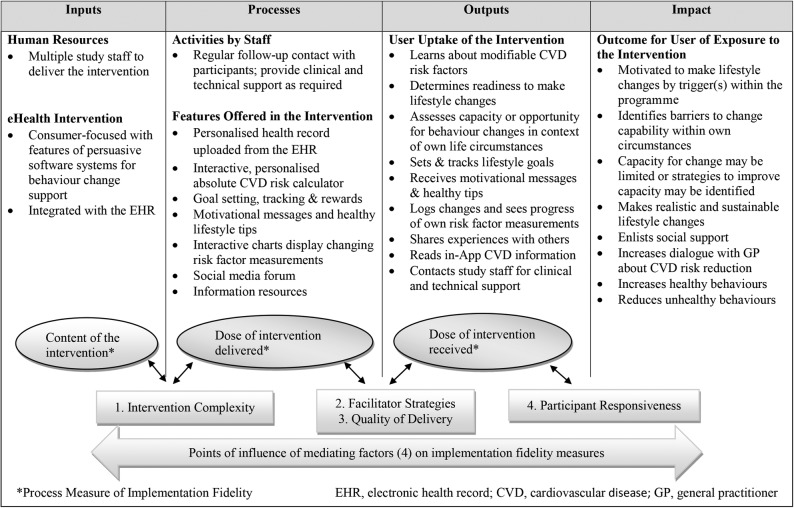
Technology-mediated strategies have potential to engage patients in modifying unhealthy behaviour and improving medication adherence to reduce morbidity and mortality from cardiovascular disease (CVD). Furthermore, electronic tools offer a medium by which consumers can more actively navigate personal healthcare information. Understanding how, why and among whom such strategies have an effect can help determine the requirements for implementing them at a scale. This paper aims to detail a process evaluation that will (1) assess implementation fidelity of a multicomponent eHealth intervention; (2) determine its effective features; (3) explore contextual factors influencing and maintaining user engagement; and (4) describe barriers, facilitators, preferences and acceptability of such interventions.
Mixed-methods sequential design to derive, examine, triangulate and report data from multiple sources. Quantitative data from 3 sources will help to inform both sampling and content framework for the qualitative data collection: (1) surveys of patients and general practitioners (GPs); (2) software analytics; (3) programme delivery records. Qualitative data from interviews with patients and GPs, focus groups with patients and field notes taken by intervention delivery staff will be thematically analysed. Concurrent interview data collection and analysis will enable a thematic framework to evolve inductively and inform theory building, consistent with a realistic evaluation perspective. Eligible patients are those at moderate-to-high CVD risk who were randomised to the intervention arm of a randomised controlled trial of an eHealth intervention and are contactable at completion of the follow-up period; eligible GPs are the primary healthcare providers of these patients.
Ethics approval has been received from the University of Sydney Human Research Ethics Committee and the Aboriginal Health and Medical Research Council (AH&MRC) of New South Wales. Results will be disseminated via scientific forums including peer-reviewed publications and national and international conferences.
ANZCTR 12613000715774.
技术介导的策略有潜力促使患者改变不健康行为并提高药物依从性,以降低心血管疾病(CVD)的发病率和死亡率。此外,电子工具提供了一种媒介,消费者可以借此更积极地获取个人医疗保健信息。了解这些策略如何、为何以及对哪些人产生效果,有助于确定大规模实施这些策略的要求。本文旨在详细介绍一项过程评估,该评估将:(1)评估多组件电子健康干预措施的实施保真度;(2)确定其有效特征;(3)探索影响和维持用户参与度的背景因素;(4)描述此类干预措施的障碍、促进因素、偏好和可接受性。
采用混合方法序列设计,从多个来源获取、检查、三角验证和报告数据。来自三个来源的定量数据将为定性数据收集的抽样和内容框架提供信息:(1)对患者和全科医生(GP)的调查;(2)软件分析;(3)项目实施记录。对患者和全科医生的访谈、患者焦点小组讨论以及干预实施人员的现场记录所获得的定性数据将进行主题分析。同步进行访谈数据收集和分析将使主题框架能够归纳发展,并为理论构建提供信息,这与现实评估视角一致。符合条件的患者是那些心血管疾病风险为中度至高度的患者,他们被随机分配到一项电子健康干预随机对照试验的干预组,并且在随访期结束时可以联系到;符合条件的全科医生是这些患者的初级医疗保健提供者。
已获得悉尼大学人类研究伦理委员会以及新南威尔士州原住民健康与医学研究理事会(AH&MRC)的伦理批准。研究结果将通过科学论坛进行传播,包括同行评审出版物以及国内和国际会议。
ANZCTR 12613000715774。