Konuma Hironori, Matsumoto Kenshi, Ueyama Hiroya, Komori Hiroyuki, Akazawa Yoichi, Ueyama Misuzu, Nakagawa Yuta, Morimoto Takashi, Takeda Tsutomu, Matsumoto Kohei, Asaoka Daisuke, Hojo Mariko, Nagahara Akihito, Yao Takashi, Miyazaki Akihisa, Watanabe Sumio
Department of Gastroenterology, Juntendo Nerima Hospital, Tokyo, Japan.
Department of Gastroenterology, Juntendo University School of Medicine, Tokyo, Japan.
Gastroenterol Res Pract. 2016;2016:9183793. doi: 10.1155/2016/9183793. Epub 2016 Dec 19.
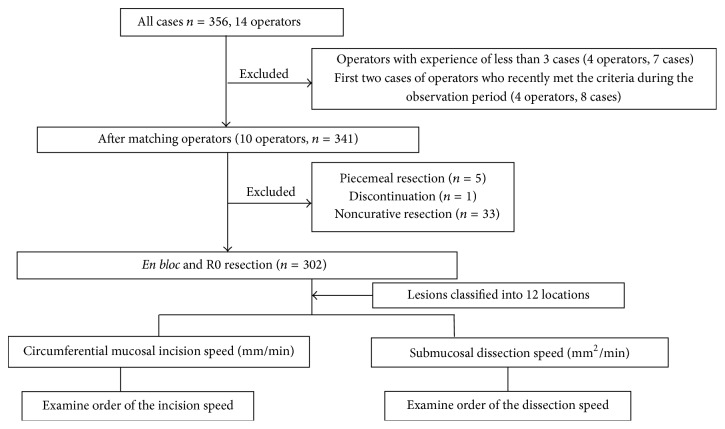
. Previous assessments of technical difficulty and procedure time for endoscopic submucosal dissection (ESD) of gastric neoplasms did not take into account several critical determinants of these parameters. However, two key phases of ESD determine the total procedure time: the mucosal circumference incision speed (CIS) and submucosal dissection speed (SDS). . We included 302 cases of and R0 resection of gastric neoplasms performed by 10 operators who had completed the training program at our hospital. Twelve locations were classified based on multiple criteria, such as condition of surrounding mucosa, lesion vascularity, presence of submucosal fat, ulcers, scars, fibrosis, and scope and device maneuverability. Lesions in different locations were classified into three groups based on the length of the procedure: fast, moderate, or late. . A significant difference was found in CIS and SDS for each location ( < 0.01), which demonstrates the validity of this classification system. In several locations, CIS and SDS were not consistent with each other. . CIS and SDS did not correspond to each other even for lesions in the same location. Consideration of ESD procedure time for gastric neoplasms requires a more elaborate classification system than that previously reported.
以往对胃肿瘤内镜黏膜下剥离术(ESD)技术难度和手术时间的评估未考虑这些参数的几个关键决定因素。然而,ESD的两个关键阶段决定了总手术时间:黏膜圆周切割速度(CIS)和黏膜下剥离速度(SDS)。我们纳入了由在我院完成培训项目的10名操作者进行的302例胃肿瘤R0切除病例。根据多个标准对12个部位进行分类,这些标准包括周围黏膜状况、病变血管情况、黏膜下脂肪的存在、溃疡、瘢痕、纤维化以及操作范围和器械可操作性。根据手术时间长短,将不同部位的病变分为三组:快速、中度或缓慢。各部位的CIS和SDS存在显著差异(P<0.01),这证明了该分类系统的有效性。在几个部位,CIS和SDS并不一致。即使对于同一部位的病变,CIS和SDS也不相互对应。考虑胃肿瘤ESD手术时间需要一个比先前报道更精细的分类系统。