Pati Rituparna, Robbins Rebekkah S, Braunstein Sarah L
Spencer Cox Center for Health/Mount Sinai Institute for Advanced Medicine, New York, New York (Dr Pati); and New York City Department of Health and Mental Hygiene, New York, New York (Ms Robbins and Dr Braunstein). Dr Pati is currently at the Centers for Disease Control and Prevention, Atlanta, Georgia.
J Public Health Manag Pract. 2017 Nov/Dec;23(6):564-570. doi: 10.1097/PHH.0000000000000515.
Improving retention in care is a key element of the National HIV/AIDS Strategy (NHAS). However, definitions for measuring retention in care are not standardized.
To compare measures of retention based on both clinic visit data and HIV laboratory surveillance data.
Retrospective cohort study.
New York City (NYC), New York.
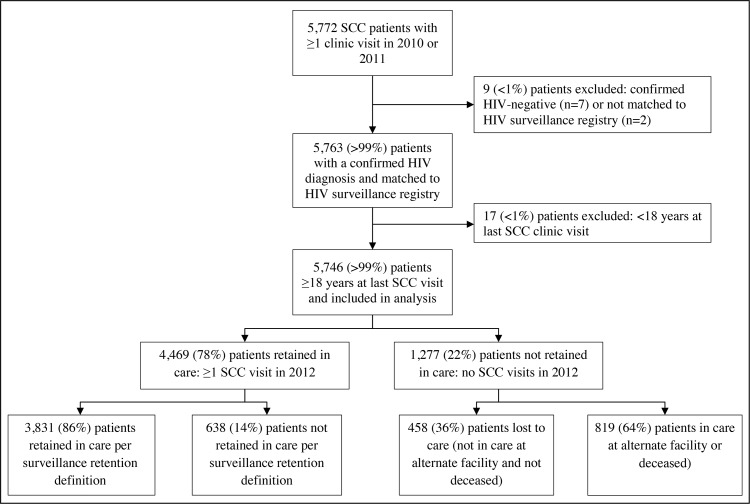
We matched adult patients with HIV infection seen at the Spencer Cox Center for Health (SCC) in 2010 or 2011 with the NYC HIV Surveillance Registry.
Retention in care was measured on the basis of SCC electronic medical record (EMR) data (≥1 medical visits in 2012) and Surveillance Registry data (≥2 CD4/viral load [VL] tests ≥90 days apart in 2012).
There were 5746 adult HIV-infected patients seen at SCC between 2010 and 2011 who matched with the Surveillance Registry. Seventy-eight percent (n = 4469) had 1 or more medical visits at SCC in 2012 and were considered retained on the basis of the EMR definition, among which 3831 (86%) met the surveillance definition for retention in care. Patients who did not have a medical visit at SCC in 2012 (n = 1277) were lost to care in NYC (n = 485; 36%), engaged in care at an alternate provider (n = 622; 49%), or died after their last SCC visit (n = 197; 15%).
This study is an important comparison of laboratory surveillance versus clinic visit-based measures of retention in care in an urban setting with the largest HIV epidemic in the country. Collaborative projects between local health departments and clinical care providers can help validate the care status of patients and inform the allocation of resources to reengage patients who are lost to care.
The combined use of laboratory and clinic visit-based data to measure retention in care provides a more accurate representation of the care status of HIV-infected patients than use of a single data source alone. Routine sharing of data by public health institutions and clinical care providers would help target resources toward reengaging patients who are lost to care in jurisdictions with universal HIV-related laboratory reporting.
提高治疗依从性是《国家艾滋病毒/艾滋病战略》(NHAS)的关键要素。然而,用于衡量治疗依从性的定义尚未标准化。
比较基于门诊就诊数据和艾滋病毒实验室监测数据的治疗依从性测量方法。
回顾性队列研究。
纽约州纽约市。
我们将2010年或2011年在斯宾塞·考克斯健康中心(SCC)就诊的成年艾滋病毒感染患者与纽约市艾滋病毒监测登记处进行了匹配。
根据SCC电子病历(EMR)数据(2012年≥1次门诊就诊)和监测登记处数据(2012年≥2次CD4/病毒载量[VL]检测,间隔≥90天)来衡量治疗依从性。
2010年至2011年期间,在SCC就诊的5746名成年艾滋病毒感染患者与监测登记处进行了匹配。78%(n = 4469)的患者在2012年在SCC有1次或更多次门诊就诊,并根据EMR定义被视为治疗依从,其中3831名(86%)符合治疗依从的监测定义。2012年未在SCC进行门诊就诊的患者(n = 1277)在纽约市失访(n = 485;36%),在其他医疗机构接受治疗(n = 622;49%),或在最后一次SCC就诊后死亡(n = 197;15%)。
本研究对该国艾滋病毒疫情最严重的城市环境中基于实验室监测与基于门诊就诊的治疗依从性测量方法进行了重要比较。地方卫生部门与临床护理提供者之间的合作项目有助于验证患者的护理状态,并为重新联系失访患者的资源分配提供信息。
与单独使用单一数据源相比,联合使用实验室数据和基于门诊就诊的数据来衡量治疗依从性能更准确地反映艾滋病毒感染患者的护理状态。公共卫生机构和临床护理提供者之间的常规数据共享将有助于将资源用于重新联系在具有普遍艾滋病毒相关实验室报告的辖区中失访的患者。