Wang Ralph C, Rodriguez Robert M, Fahimi Jahan, Hall M Kennedy, Shiboski Stephen, Chi Tom, Smith-Bindman Rebecca
Department of Emergency Medicine, University of California, San Francisco, San Francisco, CA, USA.
Department of Emergency Medicine, University of California, San Francisco, San Francisco, CA, USA.
Am J Emerg Med. 2017 Apr;35(4):554-563. doi: 10.1016/j.ajem.2016.12.009. Epub 2016 Dec 11.
Routine CT for patients with acute flank pain has not been shown to improve patient outcomes, and it may unnecessarily expose patients to radiation and increased costs. As preliminary steps toward the development of a guideline for selective CT, we sought to determine the prevalence of clinically important outcomes in patients with acute flank pain and derive preliminary decision rules.
We analyzed data from a randomized trial of CT vs. ultrasonography for patients with acute flank pain from 15 EDs between October 2011 and February 2013. Clinically important outcomes were defined as inpatient admission for ureteral stones and alternative diagnoses. Clinically important stones were defined as stones requiring urologic intervention. We sought to derive highly sensitive decision rules for both outcomes.
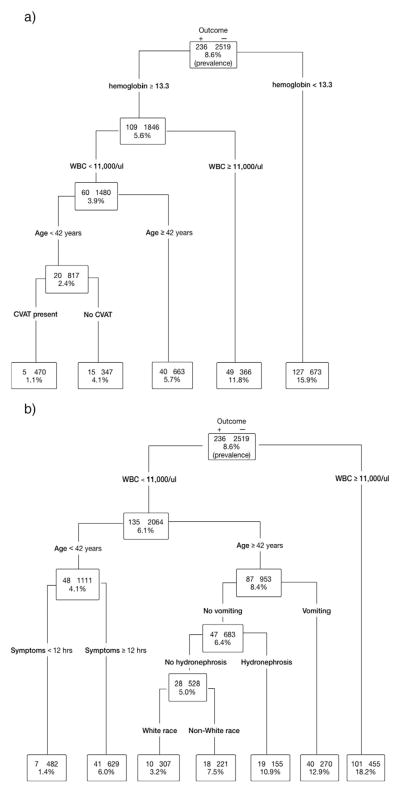
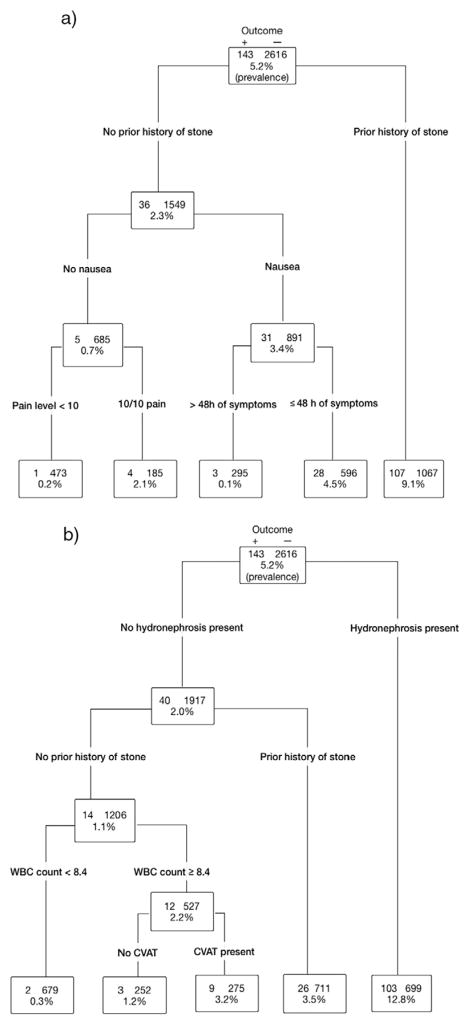
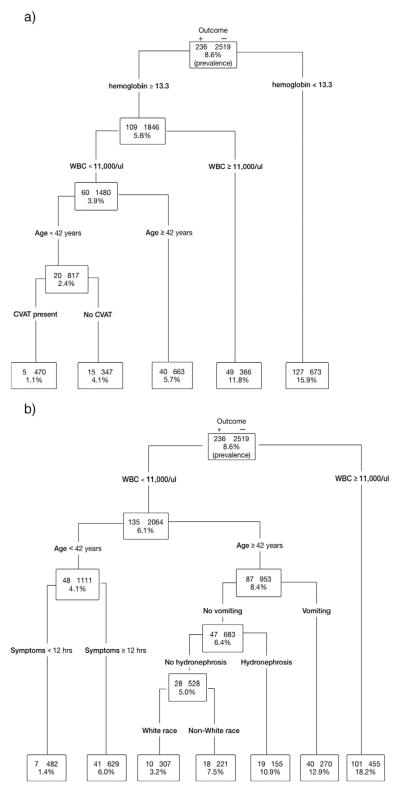
Of 2759 participants, 236 (8.6%) had a clinically important outcome and 143 (5.2%) had a clinically important stone. A CDR including anemia (hemoglobin <13.2g/dl), WBC count >11000/μl, age>42years, and the absence of CVAT had a sensitivity of 97.9% (95% CI 94.8-99.2%) and specificity of 18.7% (95% 17.2-20.2%) for clinically important outcome. A CDR including hydronephrosis, prior history of stone, and WBC count <8300/μl had a sensitivity of 98.6% (95% CI 94.5-99.7%) and specificity of 26.0% (95% 24.2-27.7%) for clinically important stone.
We determined the prevalence of clinically important outcomes in patients with acute flank pain, and derived preliminary high sensitivity CDRs that predict them. Validation of CDRs with similar test characteristics would require prospective enrollment of 2100 patients.
对于急性胁腹痛患者,常规CT检查尚未显示能改善患者预后,且可能会让患者不必要地暴露于辐射之下并增加费用。作为制定选择性CT检查指南的初步步骤,我们试图确定急性胁腹痛患者中具有临床重要意义的结局的发生率,并得出初步的决策规则。
我们分析了2011年10月至2013年2月期间15家急诊科对急性胁腹痛患者进行CT与超声检查的随机试验数据。具有临床重要意义的结局定义为因输尿管结石住院及其他诊断。具有临床重要意义的结石定义为需要泌尿外科干预的结石。我们试图得出这两种结局的高敏感性决策规则。
2759名参与者中,236人(8.6%)有具有临床重要意义的结局,143人(5.2%)有具有临床重要意义的结石。一个包含贫血(血红蛋白<13.2g/dl)、白细胞计数>11000/μl、年龄>42岁以及无肋脊角压痛的临床决策规则,对于具有临床重要意义的结局,敏感性为97.9%(95%可信区间94.8 - 99.2%),特异性为18.7%(95% 17.2 - 20.2%)。一个包含肾积水、既往结石病史以及白细胞计数<8300/μl的临床决策规则,对于具有临床重要意义的结石,敏感性为98.6%(95%可信区间94.5 - 99.7%),特异性为26.0%(95% 24.2 - 27.7%)。
我们确定了急性胁腹痛患者中具有临床重要意义的结局的发生率,并得出了预测这些结局的初步高敏感性临床决策规则。要验证具有相似检验特征的临床决策规则,需要前瞻性纳入2100名患者。