Wang Ralph C, Rodriguez Robert M, Moghadassi Michelle, Noble Vicki, Bailitz John, Mallin Mike, Corbo Jill, Kang Tarina L, Chu Phillip, Shiboski Steve, Smith-Bindman Rebecca
Department of Emergency Medicine, University of California, San Francisco, San Francisco, CA.
Department of Emergency Medicine, University of California, San Francisco, San Francisco, CA.
Ann Emerg Med. 2016 Apr;67(4):423-432.e2. doi: 10.1016/j.annemergmed.2015.08.019. Epub 2015 Oct 3.
The STONE score is a clinical decision rule that classifies patients with suspected nephrolithiasis into low-, moderate-, and high-score groups, with corresponding probabilities of ureteral stone. We evaluate the STONE score in a multi-institutional cohort compared with physician gestalt and hypothesize that it has a sufficiently high specificity to allow clinicians to defer computed tomography (CT) scan in patients with suspected nephrolithiasis.
We assessed the STONE score with data from a randomized trial for participants with suspected nephrolithiasis who enrolled at 9 emergency departments between October 2011 and February 2013. In accordance with STONE predictors, we categorized participants into low-, moderate-, or high-score groups. We determined the performance of the STONE score and physician gestalt for ureteral stone.
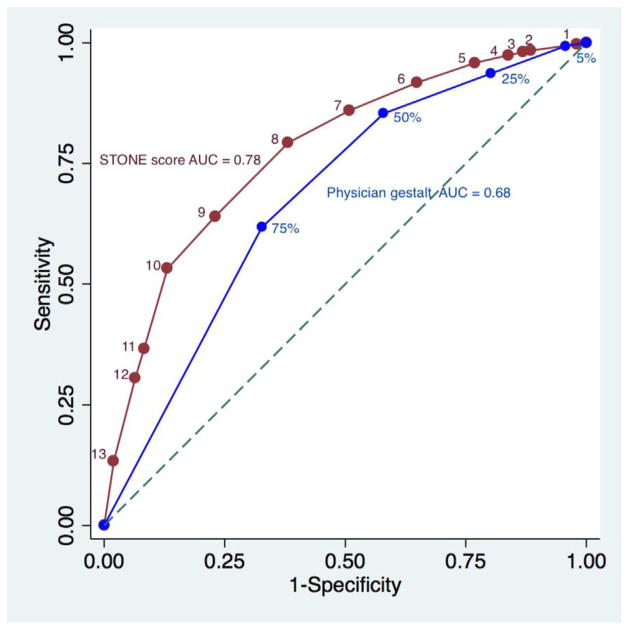
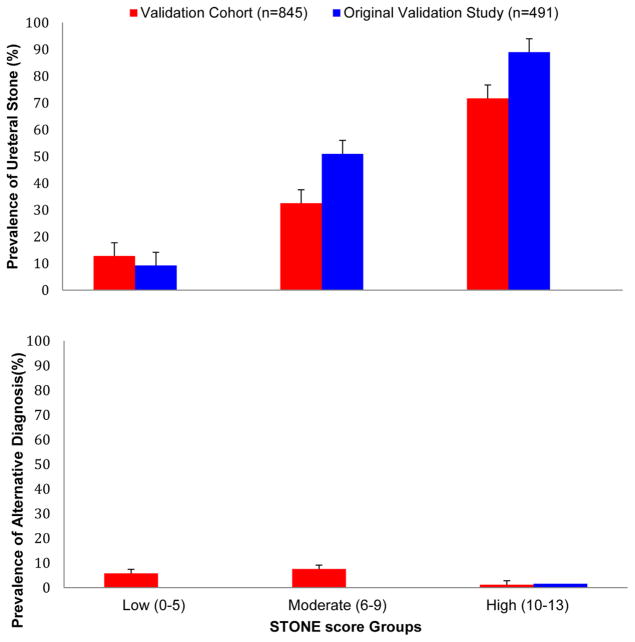
Eight hundred forty-five participants were included for analysis; 331 (39%) had a ureteral stone. The global performance of the STONE score was superior to physician gestalt (area under the receiver operating characteristic curve=0.78 [95% confidence interval {CI} 0.74 to 0.81] versus 0.68 [95% CI 0.64 to 0.71]). The prevalence of ureteral stone on CT scan ranged from 14% (95% CI 9% to 19%) to 73% (95% CI 67% to 78%) in the low-, moderate-, and high-score groups. The sensitivity and specificity of a high score were 53% (95% CI 48% to 59%) and 87% (95% CI 84% to 90%), respectively.
The STONE score can successfully aggregate patients into low-, medium-, and high-risk groups and predicts ureteral stone with a higher specificity than physician gestalt. However, in its present form, the STONE score lacks sufficient accuracy to allow clinicians to defer CT scan for suspected ureteral stone.
STONE评分是一种临床决策规则,可将疑似肾结石患者分为低分、中分和高分三组,并给出输尿管结石的相应概率。我们在一个多机构队列中评估STONE评分,并与医生的经验判断进行比较,假设其具有足够高的特异性,使临床医生能够在疑似肾结石患者中推迟进行计算机断层扫描(CT)。
我们使用2011年10月至2013年2月期间在9个急诊科登记的疑似肾结石参与者的随机试验数据评估STONE评分。根据STONE预测指标,我们将参与者分为低分、中分或高分三组。我们确定了STONE评分和医生经验判断对输尿管结石的诊断性能。
845名参与者纳入分析;331名(39%)有输尿管结石。STONE评分的整体性能优于医生的经验判断(受试者操作特征曲线下面积=0.78[95%置信区间{CI}0.74至0.81],而医生经验判断为0.68[95%CI 0.64至0.71])。低分、中分和高分三组中CT扫描显示输尿管结石的患病率分别为14%(95%CI 9%至19%)至73%(95%CI 67%至78%)。高分的敏感性和特异性分别为53%(95%CI 48%至59%)和87%(95%CI 84%至90%)。
STONE评分可以成功地将患者分为低、中、高风险组,并且比医生的经验判断更具特异性地预测输尿管结石。然而,以目前的形式,STONE评分缺乏足够的准确性,无法让临床医生为疑似输尿管结石患者推迟CT扫描。