Zhang Wei-Feng, Zhang Tuo, Ding Ding, Sun Shi-Qun, Wang Xiao-Lei, Chu Shi-Chun, Shen Ling-Hong, He Ben
Department of Cardiology, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China.
Department of Biostatistics, Johns Hopkins University, Baltimore, MD.
J Am Heart Assoc. 2017 Jan 13;6(1):e004747. doi: 10.1161/JAHA.116.004747.
Contrast-induced acute kidney injury (CI-AKI) was traditionally defined as an increase in serum creatinine (sCr) after contrast media exposure. Recently, serum cystatin C (sCyC) has been proposed as an alternative to detect acute changes in renal function. The clinical implications of combining sCyC and sCr to diagnose CI-AKI remain unknown.
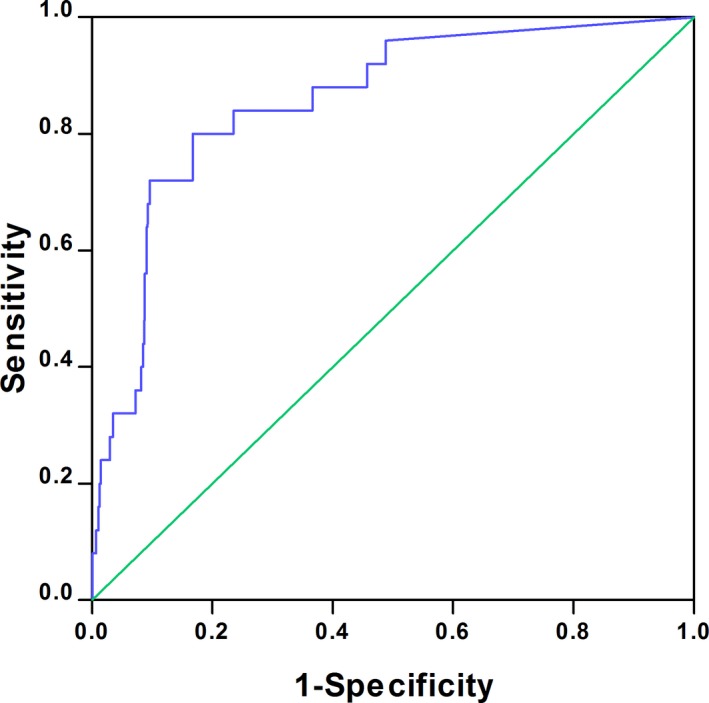
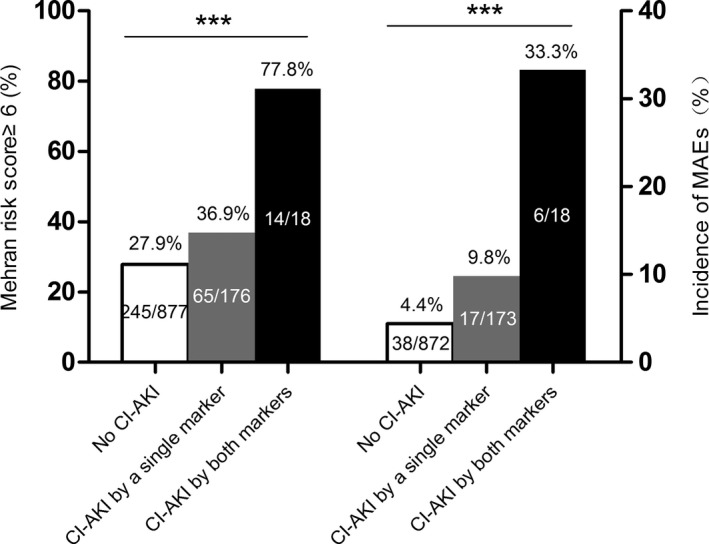
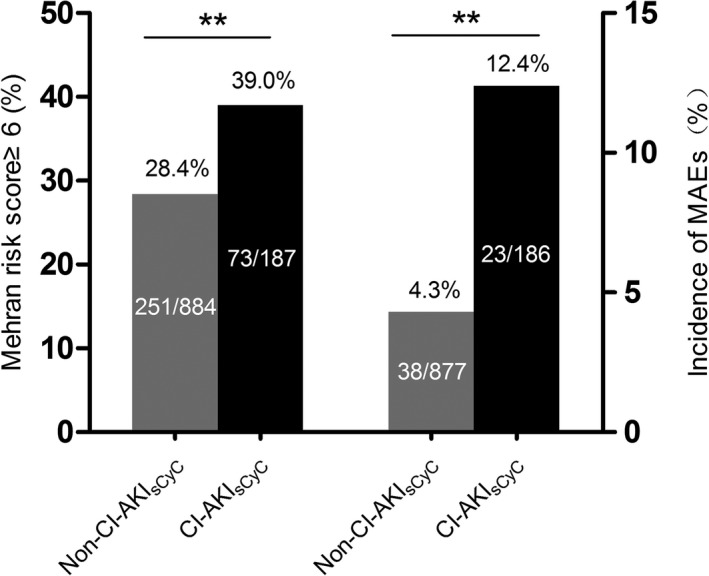
One thousand seventy-one consecutive patients undergoing coronary angiography/intervention were prospectively enrolled. SCyC and sCr were assessed at baseline and 24 to 48 hours after contrast media exposure. CI-AKI determined by sCr (CI-AKI) was defined as an sCr increase greater than 0.3 mg/dL or 50% from baseline. Major adverse events at 12 months were assessed. CI-AKI developed in 25 patients (2.3%). Twelve-month follow-up was available for 1063 patients; major adverse events occurred in 61 patients (5.7%). By receiver operating characteristic curve analysis, an sCyC increase of greater than 15% was the optimal cutoff for CI-AKI detection, which occurred in 187 patients (17.4%). To evaluate the use of both sCyC and sCr as CI-AKI diagnostic criteria, we stratified patients into 3 groups: no CI-AKI, CI-AKI detected by a single marker, and CI-AKI detected by both markers. Multivariable logistic regression revealed that the predictability of major adverse events increased in a stepwise fashion in the 3 groups (no-CI-AKI group as the reference, CI-AKI detected by a single marker: odds ratio=2.25, 95% CI: 1.24-4.10, P<0.01; CI-AKI detected by both markers: odds ratio=10.00, 95% CI: 3.13-31.91, P<0.001).
Combining sCyC and sCr to diagnose CI-AKI would be beneficial for risk stratification and prognosis in patients after contrast media exposure.
对比剂诱导的急性肾损伤(CI-AKI)传统上被定义为对比剂暴露后血清肌酐(sCr)升高。最近,血清胱抑素C(sCyC)已被提议作为检测肾功能急性变化的替代指标。联合sCyC和sCr诊断CI-AKI的临床意义尚不清楚。
前瞻性纳入1071例连续接受冠状动脉造影/介入治疗的患者。在基线以及对比剂暴露后24至48小时评估sCyC和sCr。由sCr确定的CI-AKI(CI-AKI)定义为sCr较基线升高大于0.3mg/dL或升高50%。评估12个月时的主要不良事件。25例患者(2.3%)发生了CI-AKI。1063例患者有12个月的随访数据;61例患者(5.7%)发生了主要不良事件。通过受试者工作特征曲线分析,sCyC升高大于15%是检测CI-AKI的最佳截断值,187例患者(17.4%)出现该情况。为评估同时使用sCyC和sCr作为CI-AKI诊断标准的情况,我们将患者分为3组:无CI-AKI、单一标志物检测到的CI-AKI以及两种标志物均检测到的CI-AKI。多变量逻辑回归显示,3组中主要不良事件的预测性呈逐步增加(以无CI-AKI组为参照,单一标志物检测到的CI-AKI:比值比=2.25,95%可信区间:1.24-4.10,P<0.01;两种标志物均检测到的CI-AKI:比值比=10.00,95%可信区间:3.13-31.91,P<0.001)。
联合sCyC和sCr诊断CI-AKI对对比剂暴露后患者的风险分层和预后有益。