Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan.
Department of Emergency Medicine, School of Medicine, Chung Shan Medical University, Taichung, Taiwan.
BMJ Open. 2017 Jan 13;7(1):e013029. doi: 10.1136/bmjopen-2016-013029.
Isolated minor rib fractures (IMRFs) after blunt chest traumas are commonly observed in emergency departments. However, the relationship between IMRFs and subsequent pneumonia remains controversial. This nationwide cohort study investigated the association between IMRFs and the risk of pneumonia in patients with blunt chest traumas.
Nationwide population-based cohort study.
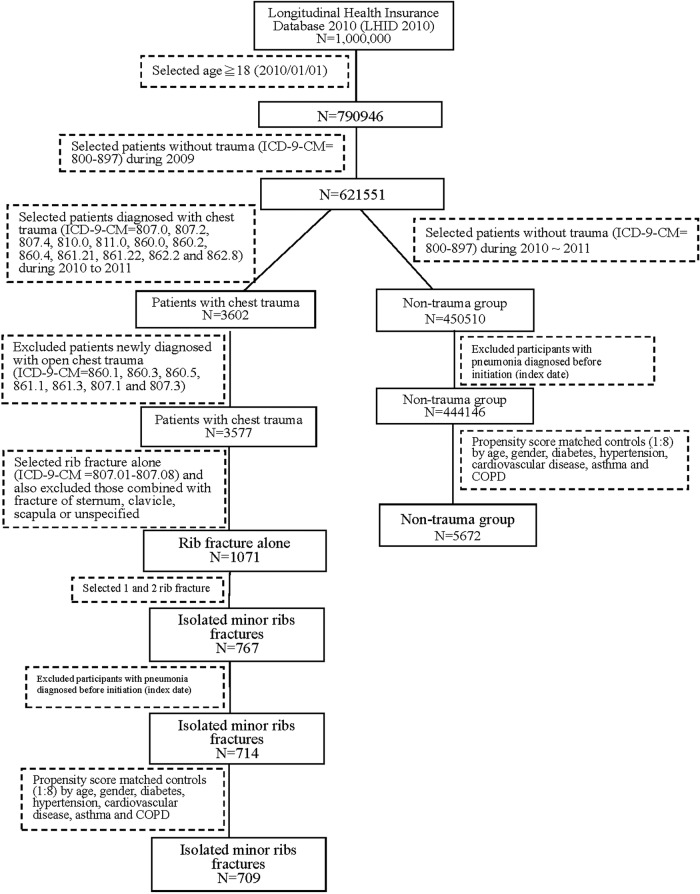
Patients with IMRFs were identified between 2010 and 2011 from the Taiwan National Health Insurance Research Database.
Non-traumatic patients were matched through 1:8 propensity-score matching according to age, sex, and comorbidities (namely diabetes, hypertension, cardiovascular disease, asthma and chronic obstructive pulmonary disease (COPD)) with the comparison cohort. We estimated the adjusted HRs (aHRs) by using the Cox proportional hazard model. A total of 709 patients with IMRFs and 5672 non-traumatic patients were included.
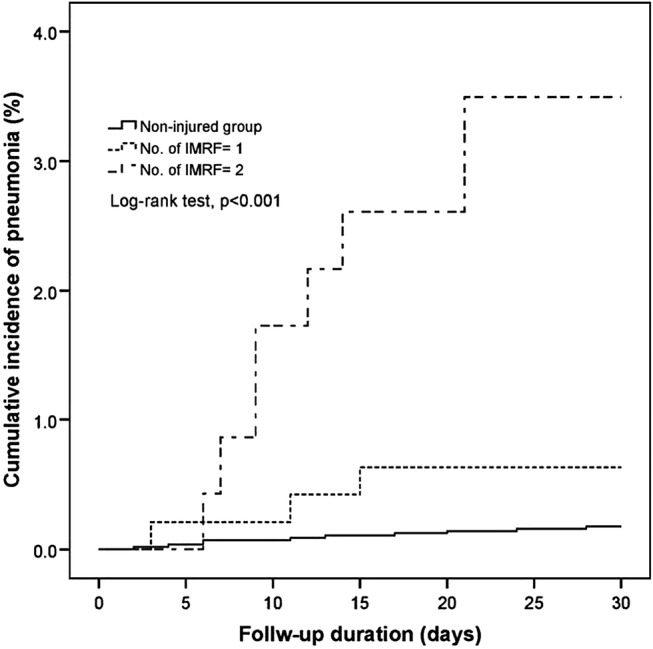
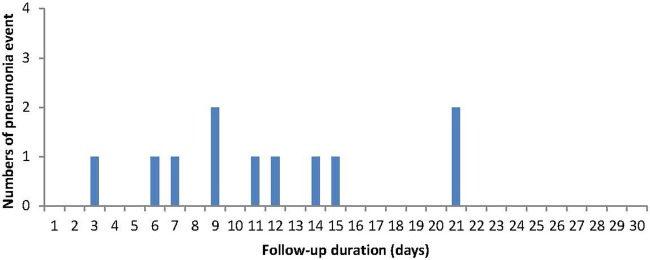
The primary end point was the occurrence of pneumonia within 30 days.
The incidence of pneumonia following IMRFs was 1.6% (11/709). The aHR for the risk of pneumonia after IMRFs was 8.94 (95% CI=3.79 to 21.09, p<0.001). Furthermore, old age (≥65 years; aHR=5.60, 95% CI 1.97 to 15.89, p<0.001) and COPD (aHR=5.41, 95% CI 1.02 to 3.59, p<0.001) were risk factors for pneumonia following IMRFs. In the IMRF group, presence of single or two isolated rib fractures was associated with an increased risk of pneumonia with aHRs of 3.97 (95% CI 1.09 to 14.44, p<0.001) and 17.13 (95% CI 6.66 to 44.04, p<0.001), respectively.
Although the incidence of pneumonia following IMRFs is low, patients with two isolated rib fractures were particularly susceptible to pneumonia. Physicians should focus on this complication, particularly in elderly patients and those with COPD.
钝性胸部外伤后孤立性肋骨骨折(IMRFs)在急诊科中较为常见。然而,IMRFs 与随后发生肺炎之间的关系仍存在争议。本全国性队列研究旨在探讨 IMRFs 与钝性胸部外伤患者发生肺炎的风险之间的关系。
全国范围内基于人群的队列研究。
从台湾全民健康保险研究数据库中,于 2010 年至 2011 年期间确定了 IMRFs 患者。
根据年龄、性别和合并症(即糖尿病、高血压、心血管疾病、哮喘和慢性阻塞性肺疾病(COPD)),通过 1:8 的倾向评分匹配,将非创伤性患者与对照队列进行匹配。我们使用 Cox 比例风险模型估计了调整后的 HR(aHR)。共纳入了 709 例 IMRFs 患者和 5672 例非创伤性患者。
主要终点为 30 天内发生肺炎。
IMRFs 后肺炎的发生率为 1.6%(11/709)。IMRFs 后发生肺炎的 aHR 为 8.94(95%CI=3.79 至 21.09,p<0.001)。此外,年龄较大(≥65 岁;aHR=5.60,95%CI 1.97 至 15.89,p<0.001)和 COPD(aHR=5.41,95%CI 1.02 至 3.59,p<0.001)是 IMRFs 后发生肺炎的危险因素。在 IMRF 组中,单一或两处孤立肋骨骨折与肺炎风险增加相关,aHR 分别为 3.97(95%CI 1.09 至 14.44,p<0.001)和 17.13(95%CI 6.66 至 44.04,p<0.001)。
尽管 IMRFs 后肺炎的发生率较低,但两处孤立性肋骨骨折的患者尤其容易发生肺炎。医生应关注这一并发症,特别是在老年患者和 COPD 患者中。