Evans Rhys D R, Hemmilä Ulla, Craik Alison, Mtekateka Mwayi, Hamilton Fergus, Kawale Zuze, Kirwan Christopher J, Dobbie Hamish, Dreyer Gavin
Department of Medicine, College of Medicine, Blantyre, Malawi.
Department of Nephrology, Queen Elizabeth Central Hospital (QECH), Blantyre, Malawi.
BMC Nephrol. 2017 Jan 14;18(1):21. doi: 10.1186/s12882-017-0446-4.
Epidemiological data on Acute Kidney Injury (AKI) from low-income countries is sparse. The aim of this study was to establish the incidence, severity, aetiology, and outcomes of community-acquired AKI in Malawi.
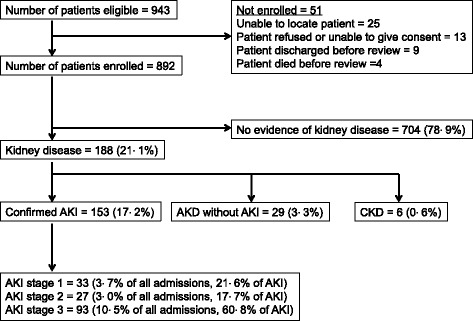
We conducted a prospective observational study of general medical admissions to a tertiary hospital in Blantyre between 27 April and 17 July 2015. All patients were screened on admission with a serum creatinine; those with creatinine above laboratory reference range were managed by the nephrology team. Hospital outcome was recorded in all patients.
Eight hundred ninety-two patients were included; 188 (21 · 1%) had kidney disease on admission, including 153 (17 · 2%) with AKI (median age 41 years; 58 · 8% HIV seropositive). 60 · 8% of AKI was stage 3. The primary causes of AKI were sepsis and hypovolaemia in 133 (86 · 9%) cases, most commonly gastroenteritis (n = 29; 19 · 0%) and tuberculosis (n = 18; 11 · 8%). AKI was multifactorial in 117 (76 · 5%) patients; nephrotoxins were implicated in 110 (71 · 9%). Inpatient mortality was 44 · 4% in patients with AKI and 13 · 9% if no kidney disease (p <0.0001). 63 · 2% of patients who recovered kidney function left hospital with persistent kidney injury.
AKI incidence is 17 · 2% in medical admissions in Malawi, the majority is severe, and AKI leads to significantly increased in-hospital mortality. The predominant causes are infection and toxin related, both potentially avoidable and treatable relatively simply. Effective interventions are urgently required to reduce preventable young deaths from AKI in this part of the world.
来自低收入国家的急性肾损伤(AKI)流行病学数据匮乏。本研究旨在确定马拉维社区获得性AKI的发病率、严重程度、病因及预后。
我们对2015年4月27日至7月17日期间布兰太尔一家三级医院的普通内科住院患者进行了一项前瞻性观察研究。所有患者入院时均进行血清肌酐筛查;肌酐高于实验室参考范围的患者由肾病团队管理。记录所有患者的医院结局。
共纳入892例患者;188例(21.1%)入院时患有肾脏疾病,其中153例(17.2%)患有AKI(中位年龄41岁;58.8% HIV血清学阳性)。60.8%的AKI为3期。AKI的主要病因是败血症和低血容量血症,共133例(86.9%),最常见的是胃肠炎(n = 29;19.0%)和结核病(n = 18;11.8%)。117例(76.5%)患者的AKI是多因素导致的;110例(71.9%)涉及肾毒素。AKI患者的住院死亡率为44.4%,无肾脏疾病患者为13.9%(p < 0.0001)。肾功能恢复的患者中有63.2%出院时仍存在持续性肾损伤。
在马拉维的内科住院患者中,AKI发病率为17.2%,大多数病情严重,且AKI导致住院死亡率显著增加。主要病因与感染和毒素相关,两者都具有潜在的可避免性且相对易于治疗。迫切需要有效的干预措施来减少世界这一地区因AKI导致的可预防的年轻死亡。