Evans Rhys D R, Sharma Sanjib K, Claure-Del Granado Rolando, Cullis Brett, Burdmann Emmanuel A, Franca Fos, Aguiar Junio, Fredlund Martyn, Hendricks Kelly, Iturricha-Caceres Maria F, Rai Mamit, Shah Bhupendra, Kafle Shyam, Harris David C, Rocco Mike V
Centre for Kidney and Bladder Health, University College London, London, United Kingdom.
B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
PLoS Med. 2024 Nov 14;21(11):e1004495. doi: 10.1371/journal.pmed.1004495. eCollection 2024 Nov.
The International Society of Nephrology proposes an acute kidney disease (AKD) management strategy that includes a risk score to aid AKD identification in low- and low-middle-income countries (LLMICs). We investigated the performance of the risk score and determined kidney and patient outcomes from AKD at multiple LLMIC sites.
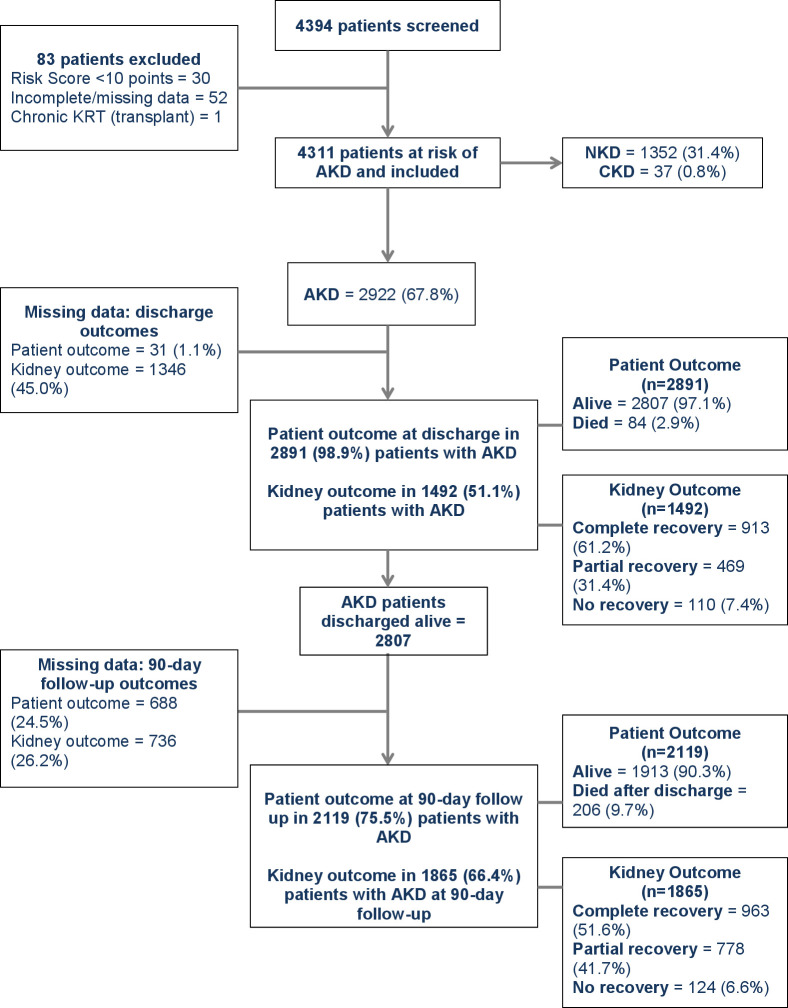
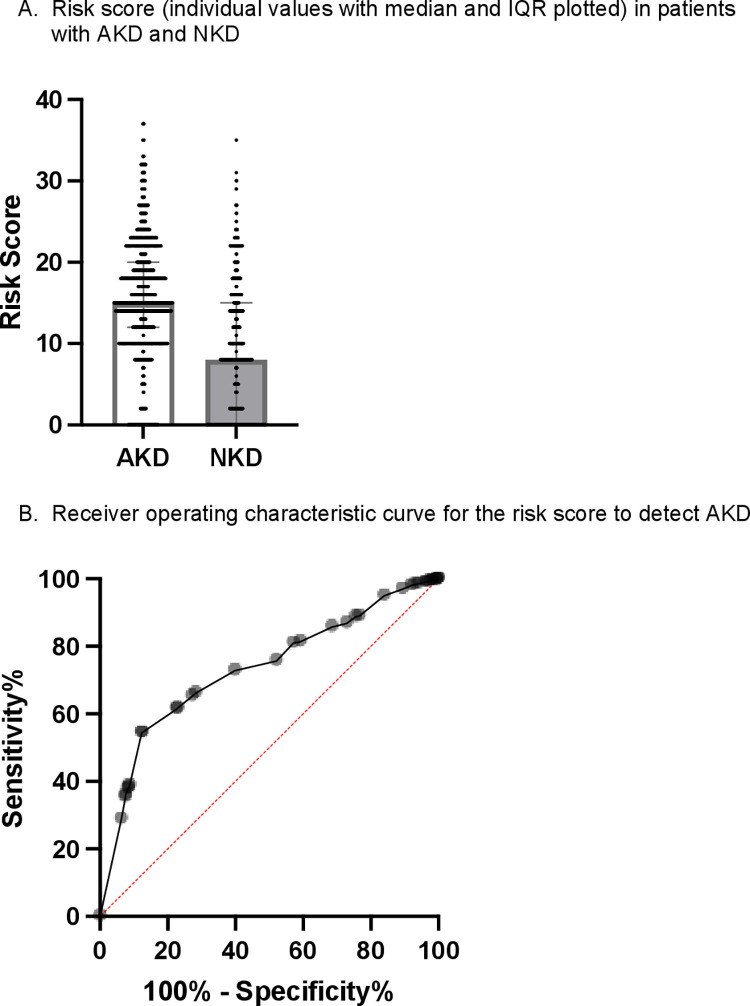
Adult patients presenting to healthcare facilities in Bolivia, Brazil, South Africa, and Nepal were screened using a symptom-based risk score and clinical judgment. Those at AKD risk underwent serum creatinine testing, predominantly with a point-of-care (POC) device. Clinical data were collected prospectively between September 2018 and November 2020. We analyzed risk score performance and determined AKD outcomes at discharge and over follow-up of 90 days. A total of 4,311 patients were at increased risk of AKD, and 2,922 (67.8%) had AKD confirmed. AKD prevalence was 80.2% in patients enrolled based on the risk score and 32.5% when enrolled on clinical judgment alone (p < 0.0001). The area under the receiver operating characteristic curve was 0.73 for the risk score to detect AKD. Death during admission occurred in 84 (2.9%) patients with AKD and 3 (0.2%) patients without kidney disease (p < 0.0001). Death after discharge occurred in 206 (9.7%) AKD patients, and 1865 AKD patients underwent reassessment of kidney function after discharge; 902 (48.4%) patients had persistent kidney disease including 740 (39.7%) patients reclassified with de novo or previously undiagnosed chronic kidney disease (CKD). The study was pragmatically designed to assess outcomes as part of routine healthcare, and there was heterogeneity in clinical practice and outcomes between sites, in addition to selection bias during cohort identification.
The use of a risk score can aid AKD identification in LLMICs. High rates of persistent kidney disease and mortality after discharge highlight the importance of AKD follow-up in low-resource settings.
国际肾脏病学会提出了一种急性肾脏病(AKD)管理策略,其中包括一个风险评分,以帮助在低收入和中低收入国家(LLMICs)识别AKD。我们调查了该风险评分的性能,并确定了多个LLMICs地点AKD患者的肾脏和患者结局。
对在玻利维亚、巴西、南非和尼泊尔的医疗机构就诊的成年患者,使用基于症状的风险评分和临床判断进行筛查。有AKD风险的患者接受血清肌酐检测,主要使用即时检测(POC)设备。在2018年9月至2020年11月期间前瞻性收集临床数据。我们分析了风险评分的性能,并确定了出院时及90天随访期内的AKD结局。共有4311名患者有增加的AKD风险,其中2922名(67.8%)被确诊为AKD。基于风险评分入组的患者中AKD患病率为80.2%,仅基于临床判断入组时为32.5%(p<0.0001)。风险评分检测AKD的受试者工作特征曲线下面积为0.73。84名(2.9%)AKD患者和3名(0.2%)无肾脏疾病患者在住院期间死亡(p<0.0001)。206名(9.7%)AKD患者出院后死亡,1865名AKD患者出院后接受了肾功能重新评估;902名(48.4%)患者患有持续性肾脏疾病,其中740名(39.7%)患者被重新分类为新发或先前未诊断的慢性肾脏病(CKD)。该研究旨在作为常规医疗保健的一部分对结局进行评估,除了队列识别期间的选择偏倚外,各地点的临床实践和结局也存在异质性。
使用风险评分有助于在LLMICs中识别AKD。出院后持续性肾脏疾病和死亡率较高,凸显了在资源匮乏地区进行AKD随访的重要性。