Arcopinto Michele, Salzano Andrea, Giallauria Francesco, Bossone Eduardo, Isgaard Jörgen, Marra Alberto M, Bobbio Emanuele, Vriz Olga, Åberg David N, Masarone Daniele, De Paulis Amato, Saldamarco Lavinia, Vigorito Carlo, Formisano Pietro, Niola Massimo, Perticone Francesco, Bonaduce Domenico, Saccà Luigi, Colao Annamaria, Cittadini Antonio
Dipartimento di Scienze Mediche Traslazionali, Federico II University, Naples, Italy.
Dipartimento di Cardiologia e Cardiochirurgia, University Hospital "Scuola Medica Salernitana", Salerno, Italy.
PLoS One. 2017 Jan 17;12(1):e0170058. doi: 10.1371/journal.pone.0170058. eCollection 2017.
Although mounting evidence supports the concept that growth hormone (GH) deficiency (GHD) affects cardiovascular function, no study has systematically investigated its prevalence and role in a large cohort of chronic heart failure (CHF) patients. Aim of this study is to assess the prevalence of GHD in mild-to-moderate CHF and to explore clinical and functional correlates of GHD.
One-hundred thirty CHF patients underwent GH provocative test with GHRH+arginine and accordingly categorized into GH-deficiency (GHD, n = 88, age = 61.6±1.1 years, 68% men) and GH-sufficiency (GHS, n = 42, age = 63.6±1.5 years, 81% men) cohorts. Both groups received comprehensive cardiovascular examination and underwent Doppler echocardiography, cardiopulmonary exercise testing, and biochemical and hormonal assay.
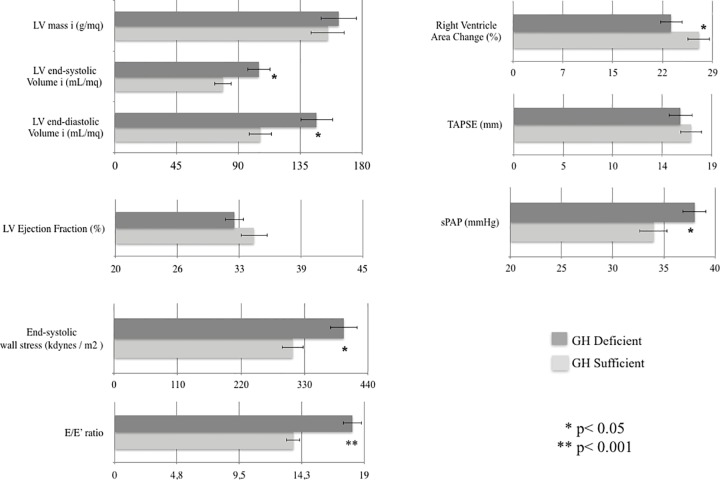
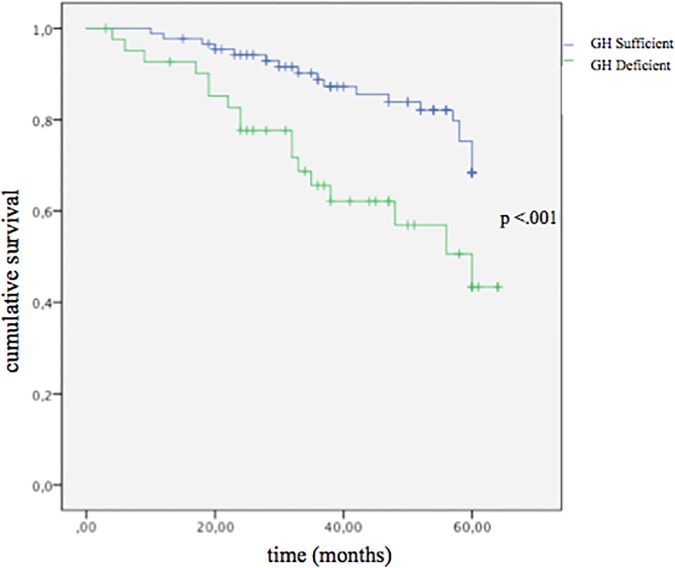
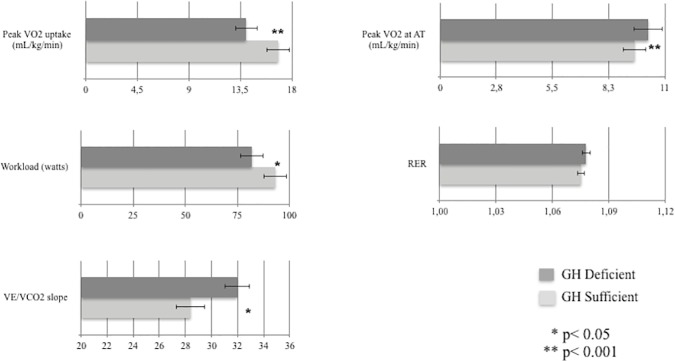
GHD was detected in roughly 30% of CHF patients. Compared to GHD, GHS patients showed smaller end-diastolic and end-systolic LV volumes (-28%, p = .008 and -24%, p = .015, respectively), lower LV end-systolic wall stress (-21%, p = .03), higher RV performance (+18% in RV area change, p = .03), lower estimated systolic pulmonary artery pressure (-11%, p = .04), higher peak VO2 (+20%, p = .001) and increased ventilatory efficiency (-12% in VE/VCO2 slope, p = .002). After adjusting for clinical covariates (age, gender, and tertiles of LV ejection fraction, IGF-1, peak VO2, VE/VCO2 slope, and NT-proBNP), logistic multivariate analysis showed that peak VO2 (β = -1.92, SE = 1.67, p = .03), VE/VCO2 slope (β = 2.23, SE = 1.20, p = .02) and NT-proBNP (β = 2.48, SE = 1.02, p = .016), were significantly associated with GHD status. Finally, compared to GHS, GHD cohort showed higher all-cause mortality at median follow-up of 3.5 years (40% vs. 25%, p < .001, respectively), independent of age, sex, NT-proBNP, peak VO2 and LVEF.
GH deficiency identifies a subgroup of CHF patients characterized by impaired functional capacity, LV remodeling and elevated NT-proBNP levels. GHD is also associated with increased all-cause mortality.
尽管越来越多的证据支持生长激素(GH)缺乏(GHD)会影响心血管功能这一概念,但尚无研究系统调查其在大量慢性心力衰竭(CHF)患者中的患病率及作用。本研究旨在评估轻至中度CHF患者中GHD的患病率,并探讨GHD的临床及功能相关性。
130例CHF患者接受了生长激素释放激素(GHRH)+精氨酸激发试验,并据此分为生长激素缺乏(GHD,n = 88,年龄 = 61.6±1.1岁,68%为男性)组和生长激素充足(GHS,n = 42,年龄 = 63.6±1.5岁,81%为男性)组。两组均接受了全面的心血管检查,并进行了多普勒超声心动图、心肺运动试验以及生化和激素检测。
约30%的CHF患者检测出GHD。与GHD组相比,GHS组患者左心室舒张末期和收缩末期容积较小(分别减少28%,p = 0.008和24%,p = 0.015),左心室收缩末期壁应力较低(降低21%,p = 0.03),右心室功能较高(右心室面积变化增加18%,p = 0.03),估计的收缩期肺动脉压较低(降低11%,p = 0.04),峰值摄氧量较高(增加20%,p = 0.001),通气效率提高(VE/VCO2斜率降低12%,p = 0.002)。在对临床协变量(年龄、性别以及左心室射血分数、胰岛素样生长因子-1、峰值摄氧量、VE/VCO2斜率和N末端脑钠肽前体的三分位数)进行校正后,逻辑多变量分析显示,峰值摄氧量(β = -1.92,标准误 = 1.67,p = 0.03)、VE/VCO2斜率(β = 2.23,标准误 = 1.20,p = 0.02)和N末端脑钠肽前体(β = 2.48,标准误 = 1.02,p = 0.016)与GHD状态显著相关。最后,与GHS组相比,GHD组在3.5年的中位随访期内全因死亡率更高(分别为40%对25%,p < 0.001),且与年龄、性别、N末端脑钠肽前体、峰值摄氧量和左心室射血分数无关。
生长激素缺乏可识别出一组CHF患者,其特征为功能能力受损、左心室重构以及N末端脑钠肽前体水平升高。GHD还与全因死亡率增加相关。