Alhamad Tarek, Malone Andrew F, Brennan Daniel C, Stratta Robert J, Chang Su-Hsin, Wellen Jason R, Horwedel Timothy A, Lentine Krista L
1 Division of Nephrology, Department of Internal Medicine, Washington University School of Medicine, St. Louis, MO. 2 Transplant Epidemiology Research Collaboration (TERC), Institute of Public Health, Washington University School of Medicine, St. Louis, MO. 3 Department of Surgery, Wake Forest School of Medicine, Winston-Salem, NC. 4 Division of Public Health Sciences, Department of Surgery, Washington University School of Medicine, St. Louis, MO. 5 Department of Surgery, Washington University School of Medicine, St. Louis, MO. 6 Department of Pharmacy, Barnes-Jewish Hospital, St. Louis, MO. 7 Saint Louis University Center for Abdominal Transplantation, Saint Louis University School of Medicine, St. Louis, MO. 8 Division of Nephrology, Department of Internal Medicine, Saint Louis University School of Medicine, St. Louis, MO.
Transplantation. 2017 Nov;101(11):2757-2764. doi: 10.1097/TP.0000000000001628.
Successful pancreas transplantation requires surgical expertise and multidisciplinary medical management. The impact of transplant center volume on pancreas allograft survival remains unclear.
We examined Organ Procurement and Transplantation Network data on 11 568 simultaneous pancreas-kidney (SPK) and 4308 solitary pancreas (pancreas transplant alone and pancreas after kidney) transplants between 2000 and 2013.
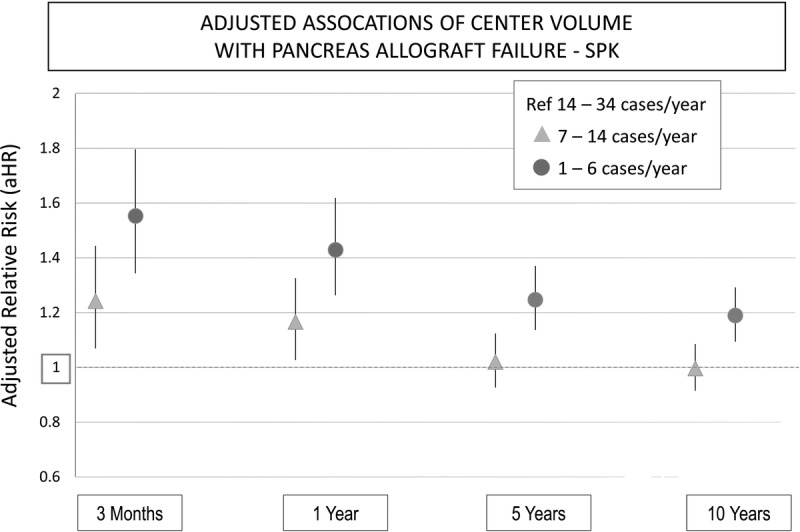
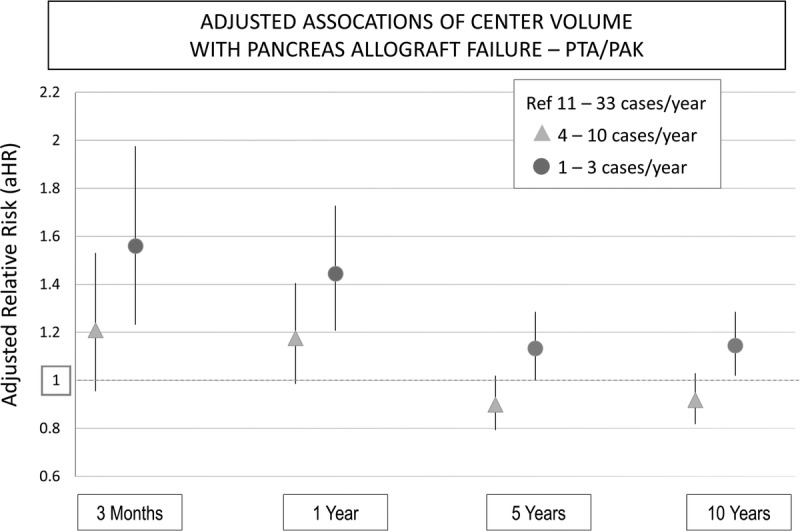
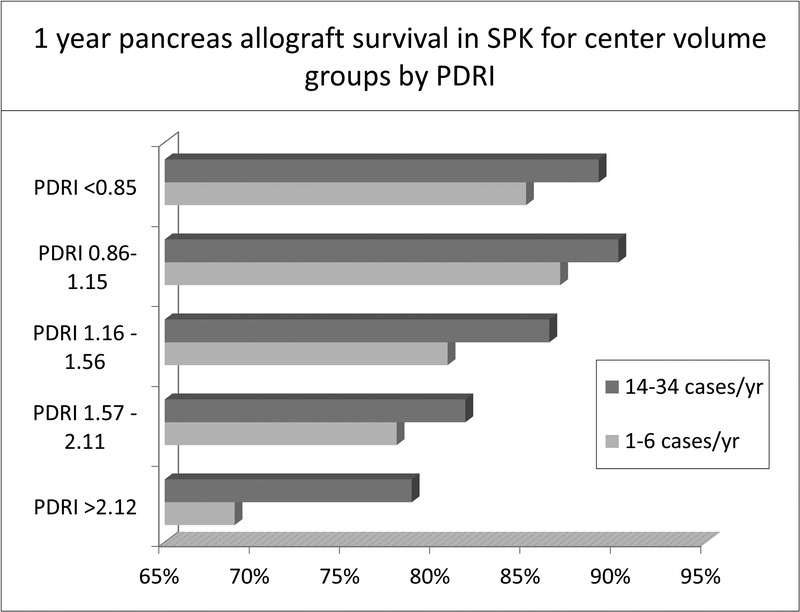
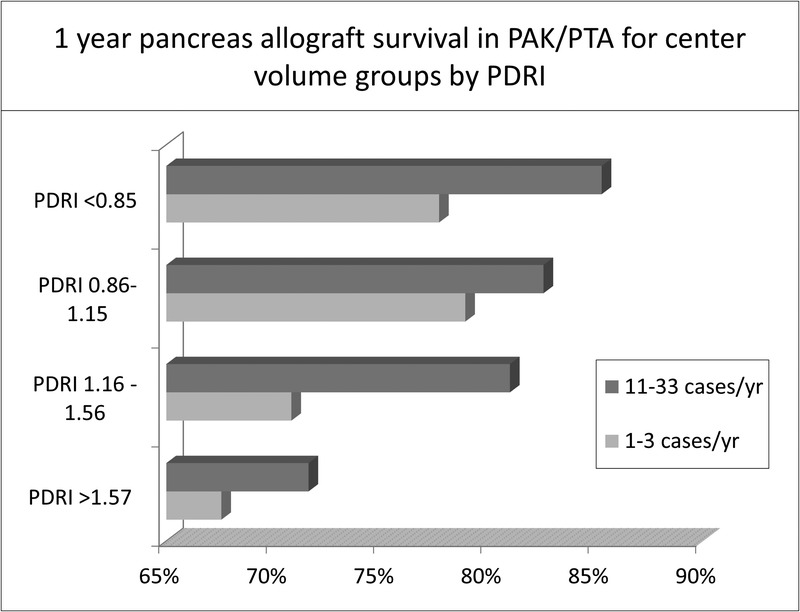
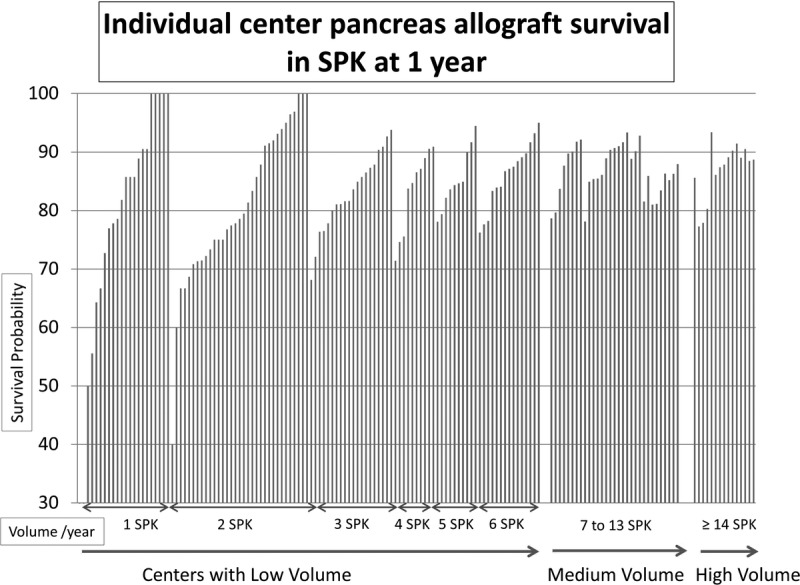
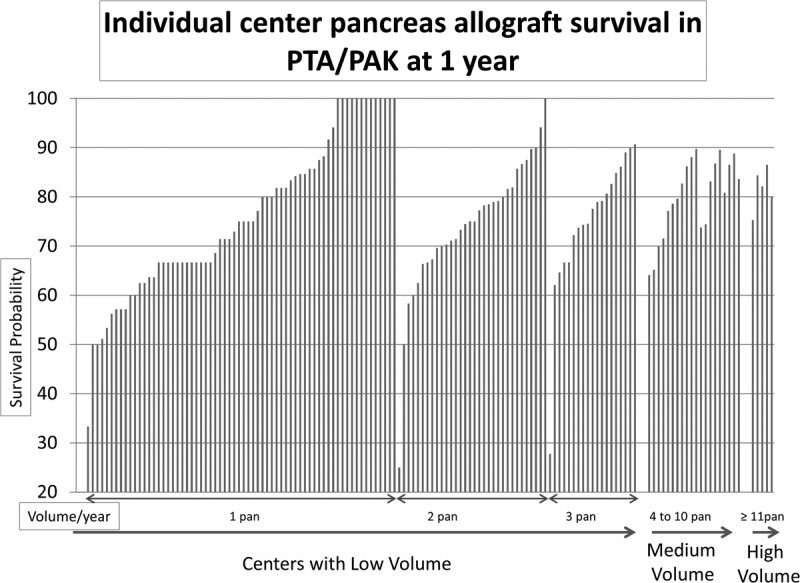
Average annual transplant center volume was categorized by tertiles into low, medium, and high volume, respectively, as follows: 1 to 6 (n = 3861), 7 to 13 (n = 3891), and 14 to 34 (n = 3888) for SPK, and 1 to 3 (n = 1417), 4 to 10 (n = 1518), and 11 to 33 (n = 1377) for solitary pancreas transplants. Favorable donor characteristics were seen in low-volume centers. For SPK transplantation, low (adjusted hazard ration [aHR], 1.55, 95% confidence interval [CI], 1.34-1.8) and medium (aHR, 1.24; 95% CI, 1.07-1.44) center volumes were associated with a higher risk of early pancreas graft failure at 3 months. The increased risk associated with low center volume extended to 1, 5, and 10 years. For solitary pancreas transplants, low, but not medium, center volume was associated with a higher risk of early pancreas graft failure at 3 months (aHR, 1.56; 95% CI, 1.232-1.976), and this risk persisted over 10 years. Patients transplanted at high-volume centers had better pancreas survival rates across all categories of the Pancreas Donor Risk Index.
On average, low center volume were associated with higher risk for pancreas failure. Future studies should seek to identify care processes that support optimal outcomes after pancreas transplantation irrespective of center volume.
成功的胰腺移植需要外科专业知识和多学科医疗管理。移植中心的手术量对胰腺移植存活率的影响尚不清楚。
我们研究了器官获取与移植网络(Organ Procurement and Transplantation Network)在2000年至2013年间的11568例胰肾联合移植(SPK)和4308例单独胰腺移植(单独胰腺移植和肾移植后胰腺移植)的数据。
移植中心的年平均手术量按三分位数分为低、中、高手术量,具体如下:SPK移植分别为1至6例(n = 3861)、7至13例(n = 3891)和14至34例(n = 3888),单独胰腺移植分别为1至3例(n = 1417)、4至10例(n = 1518)和11至33例(n = 1377)。低手术量中心的供体特征较好。对于SPK移植,低手术量(校正风险比[aHR],1.55,95%置信区间[CI],1.34 - 1.8)和中等手术量(aHR,1.24;95% CI,1.07 - 1.44)的中心在3个月时早期胰腺移植失败的风险较高。与低手术量中心相关的风险增加持续到1年、5年和10年。对于单独胰腺移植,低手术量(而非中等手术量)中心在3个月时早期胰腺移植失败的风险较高(aHR = 1.56;95% CI,1.232 - 1.976),且这种风险持续超过10年。在胰腺供体风险指数的所有类别中,高手术量中心的患者胰腺存活率更高。
平均而言,低手术量中心与胰腺移植失败的较高风险相关。未来的研究应致力于确定无论中心手术量如何都能支持胰腺移植后获得最佳结果的护理流程。