Willis Mark, Pearson Owen, Illes Zsolt, Sejbaek Tobias, Nielsen Christian, Duddy Martin, Petheram Kate, van Munster Caspar, Killestein Joep, Malmeström Clas, Tallantyre Emma, Robertson Neil
Department of Neurology (M.W., E.T., N.R.), Institute of Psychological Medicine and Clinical Neuroscience, Cardiff University, University Hospital of Wales; Department of Neurology (O.P.), Morriston Hospital, Heol Maes Eglwys, Morriston, Swansea, UK; Departments of Neurology (Z.I., T.S.) and Clinical Immunology (C.N.), Odense University Hospital, University of Southern Denmark; Department of Neurology (M.D.), The Royal Victoria Infirmary, Newcastle upon Tyne; Department of Neurology (K.P.), Sunderland Royal Hospital, UK; VU University Medical Center (C.v.M., J.K.), Amsterdam, the Netherlands; and Department of Neurology (C.M.), Sahlgrenska Academy at the University of Gothenburg, Institute of Clinical Neuroscience and Physiology, Gothenburg, Sweden.
Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10;4(2):e320. doi: 10.1212/NXI.0000000000000320. eCollection 2017 Mar.
To describe a series of patients with relapsing multiple sclerosis (MS) who experienced significant and unexpected disease activity within the first 12 months after switching from fingolimod to alemtuzumab.
Patients with relapsing MS treated sequentially with fingolimod then alemtuzumab who experienced significant subsequent disease activity were identified by personal communication with 6 different European neuroscience centers.
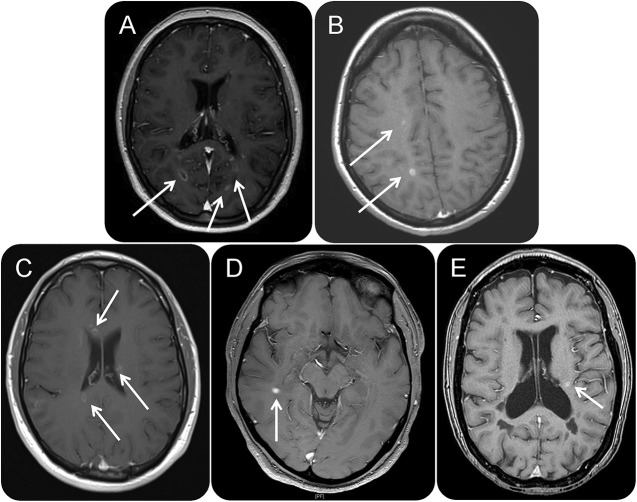
Nine patients were identified. Median disease duration to alemtuzumab treatment was 94 (39-215) months and follow-up from time of first alemtuzumab cycle 20 (14-21) months. Following first alemtuzumab infusion cycle, 8 patients were identified by at least 1 clinical relapse and radiologic disease activity and 1 by significant radiologic disease activity alone.
We acknowledge the potential for ascertainment bias; however, these cases may illustrate an important cause of reduced efficacy of alemtuzumab in a vulnerable group of patients with MS most in need of disease control. We suggest that significant and unexpected subsequent disease activity after alemtuzumab induction results from prolonged sequestration of autoreactive lymphocytes following fingolimod withdrawal, allowing these cells to be concealed from the usual biological effect of alemtuzumab. Subsequent lymphocyte egress then provokes disease reactivation. Further animal studies and clinical trials are required to confirm these phenomena and in the meantime careful consideration should be given to mode of action of individual therapies and sequential treatment effects in MS when designing personalized treatment regimens.
描述一系列复发型多发性硬化症(MS)患者,这些患者在从芬戈莫德转换为阿仑单抗后的前12个月内经历了显著且意外的疾病活动。
通过与6个不同的欧洲神经科学中心进行个人交流,识别出依次接受芬戈莫德和阿仑单抗治疗且随后出现显著疾病活动的复发型MS患者。
共识别出9例患者。接受阿仑单抗治疗的疾病持续时间中位数为94(39 - 215)个月,从首次阿仑单抗治疗周期开始的随访时间为20(14 - 21)个月。在首次阿仑单抗输注周期后,8例患者出现至少1次临床复发和影像学疾病活动,1例仅出现显著的影像学疾病活动。
我们承认存在确定偏倚的可能性;然而,这些病例可能说明了阿仑单抗在最需要疾病控制的脆弱MS患者群体中疗效降低的一个重要原因。我们认为,阿仑单抗诱导后出现显著且意外的后续疾病活动是由于停用芬戈莫德后自身反应性淋巴细胞长期隔离,使这些细胞对阿仑单抗的通常生物学效应隐匿,随后淋巴细胞流出引发疾病重新激活。需要进一步的动物研究和临床试验来证实这些现象,同时在设计个性化治疗方案时,应仔细考虑MS中个体疗法的作用方式和序贯治疗效果。