Eidel Oliver, Burth Sina, Neumann Jan-Oliver, Kieslich Pascal J, Sahm Felix, Jungk Christine, Kickingereder Philipp, Bickelhaupt Sebastian, Mundiyanapurath Sibu, Bäumer Philipp, Wick Wolfgang, Schlemmer Heinz-Peter, Kiening Karl, Unterberg Andreas, Bendszus Martin, Radbruch Alexander
Department of Neuroradiology, University of Heidelberg Medical Center, Heidelberg, Germany.
Department of Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany.
PLoS One. 2017 Jan 19;12(1):e0169292. doi: 10.1371/journal.pone.0169292. eCollection 2017.
To correlate histopathologic findings from biopsy specimens with their corresponding location within enhancing areas, non-enhancing areas and necrotic areas on contrast enhanced T1-weighted MRI scans (cT1).
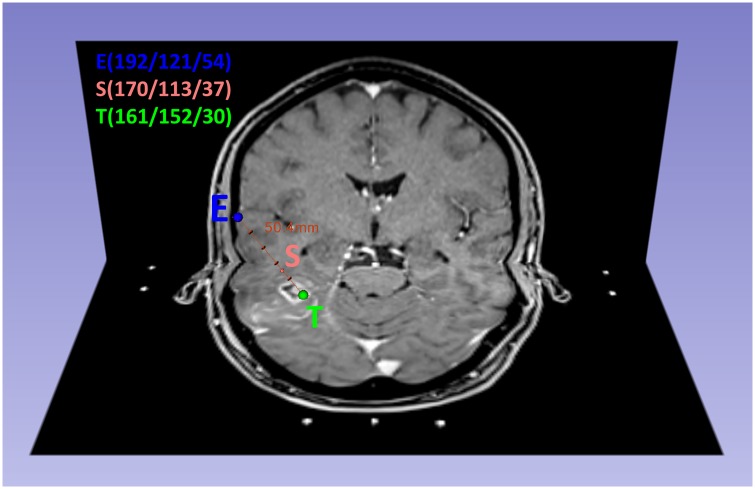
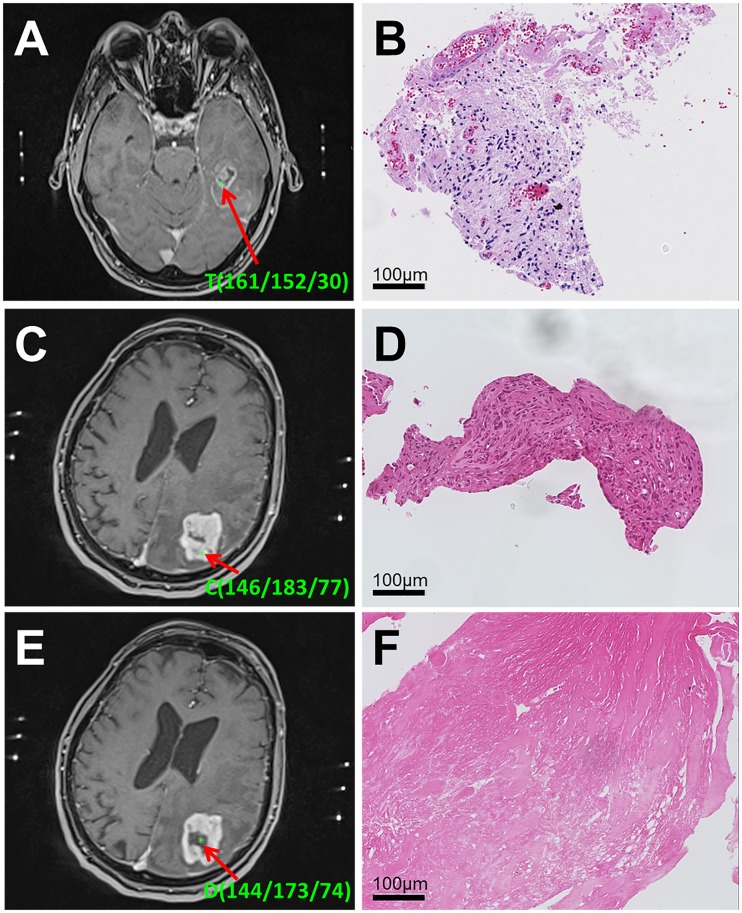
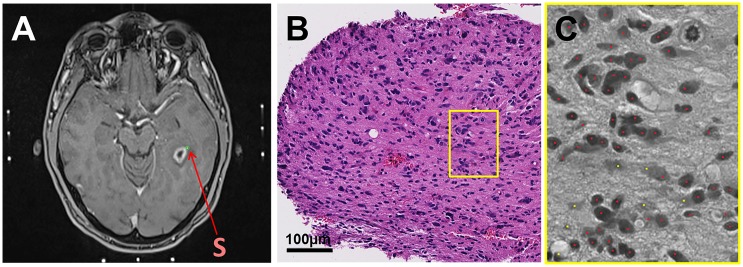
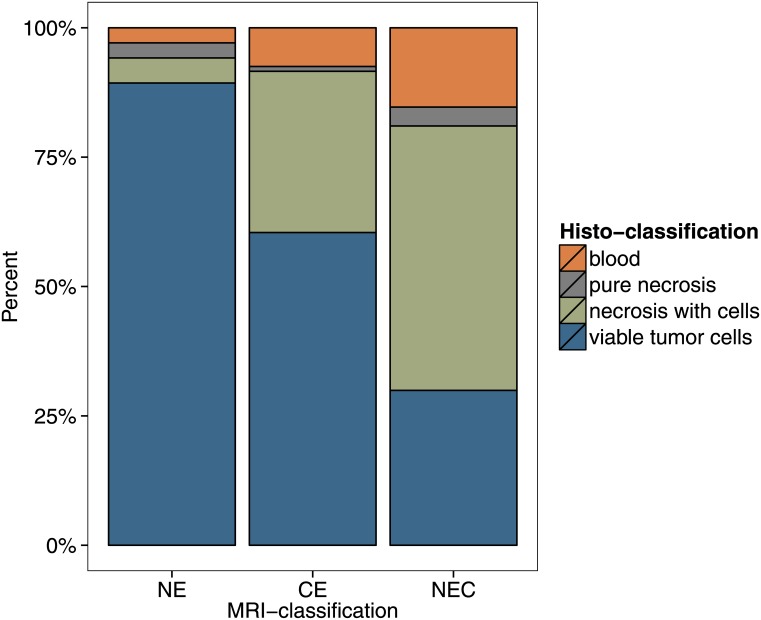
In 37 patients with newly diagnosed glioblastoma who underwent stereotactic biopsy, we obtained a correlation of 561 1mm3 biopsy specimens with their corresponding position on the intraoperative cT1 image at 1.5 Tesla. Biopsy points were categorized as enhancing (CE), non-enhancing (NE) or necrotic (NEC) on cT1 and tissue samples were categorized as "viable tumor cells", "blood" or "necrotic tissue (with or without cellular component)". Cell counting was done semi-automatically.
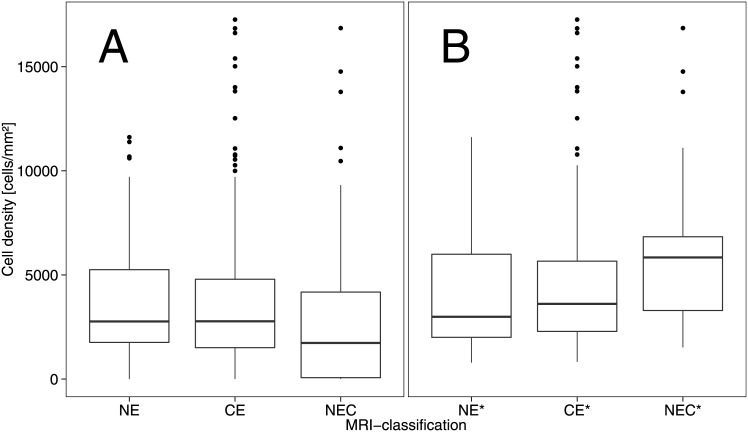
NE had the highest content of tissue categorized as viable tumor cells (89% vs. 60% in CE and 30% NEC, respectively). Besides, the average cell density for NE (3764 ± 2893 cells/mm2) was comparable to CE (3506 ± 3116 cells/mm2), while NEC had a lower cell density with 2713 ± 3239 cells/mm2. If necrotic parts and bleeds were excluded, cell density in biopsies categorized as "viable tumor tissue" decreased from the center of the tumor (NEC, 5804 ± 3480 cells/mm2) to CE (4495 ± 3209 cells/mm2) and NE (4130 ± 2817 cells/mm2).
The appearance of a glioblastoma on a cT1 image (circular enhancement, central necrosis, peritumoral edema) does not correspond to its diffuse histopathological composition. Cell density is elevated in both CE and NE parts. Hence, our study suggests that NE contains considerable amounts of infiltrative tumor with a high cellularity which might be considered in resection planning.
将活检标本的组织病理学结果与其在对比增强T1加权磁共振成像(cT1)扫描的强化区域、非强化区域和坏死区域内的相应位置相关联。
在37例接受立体定向活检的新诊断胶质母细胞瘤患者中,我们获得了561个1立方毫米活检标本与其在1.5特斯拉术中cT1图像上相应位置的相关性。活检点在cT1上分为强化(CE)、非强化(NE)或坏死(NEC),组织样本分为“存活肿瘤细胞”、“血液”或“坏死组织(有或无细胞成分)”。细胞计数采用半自动方式进行。
NE中归类为存活肿瘤细胞的组织含量最高(分别为89%,而CE中为60%,NEC中为30%)。此外,NE的平均细胞密度(3764±2893个细胞/平方毫米)与CE(3506±3116个细胞/平方毫米)相当,而NEC的细胞密度较低,为2713±3239个细胞/平方毫米。如果排除坏死部分和出血,归类为“存活肿瘤组织”的活检中的细胞密度从肿瘤中心(NEC,5804±3480个细胞/平方毫米)向CE(4495±3209个细胞/平方毫米)和NE(4130±2817个细胞/平方毫米)降低。
胶质母细胞瘤在cT1图像上的表现(环形强化、中心坏死、瘤周水肿)与其弥漫性组织病理学组成不对应。CE和NE部分的细胞密度均升高。因此,我们的研究表明,NE含有大量具有高细胞密度的浸润性肿瘤,在切除计划中可能需要考虑这一点。