Kazemi Arash, McLaren Jay W, Lin Shuai-Chun, Toris Carol B, Gulati Vikas, Moroi Sayoko E, Sit Arthur J
Department of Ophthalmology, Mayo Clinic, Rochester, Minnesota, United States.
Department of Ophthalmology and Visual Sciences, Case Western Reserve University, Cleveland, Ohio, United States 3Department of Ophthalmology and Visual Sciences, University of Nebraska Medical Center, Omaha, Nebraska, United States.
Invest Ophthalmol Vis Sci. 2017 Jan 1;58(1):204-210. doi: 10.1167/iovs.16-20754.
It is not known if outflow facilities measured by pneumatonography and Schiøtz tonography are interchangeable. In this study we compared outflow facility measured by pneumatonography to outflow facility measured by digital Schiøtz tonography.
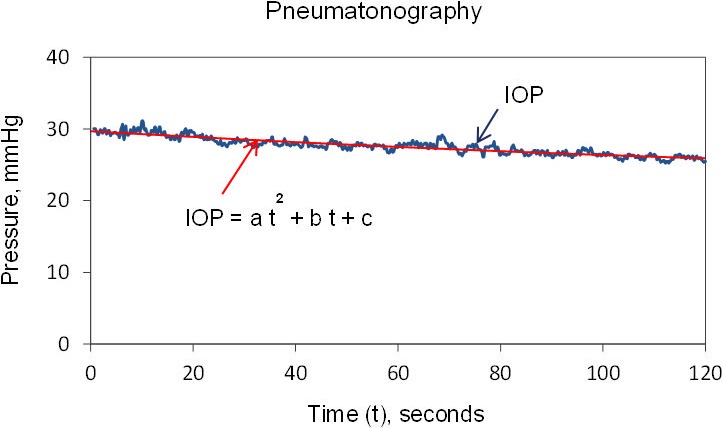
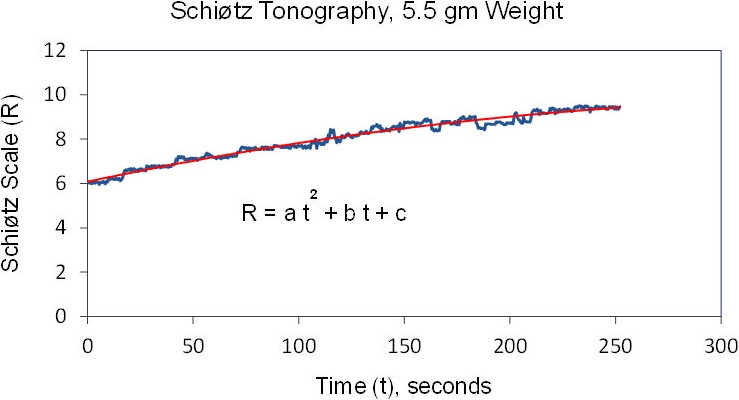
Fifty-six eyes from 28 healthy participants, ages 41 to 68 years, were included. Intraocular pressure (IOP) was measured in the sitting and supine positions with a pneumatonometer. With the subject in the supine position, IOP was recorded for 2 minutes by using a pneumatonometer with a 10-g weight and for 4 minutes by using a custom digital Schiøtz tonometer. Outflow facility was determined from the changes in pressure and intraocular volume and a standard assumed ocular rigidity coefficient for each instrument, respectively, and by using an ocular rigidity coefficient calculated by measuring pressure without and with a weight added to the pneumatonometer tip.
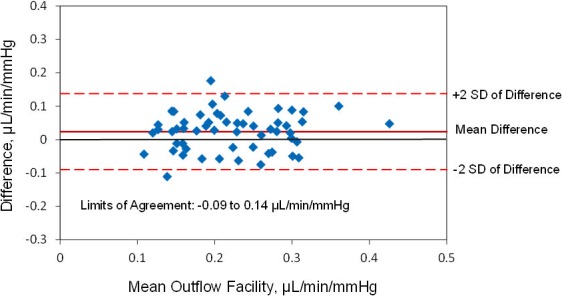
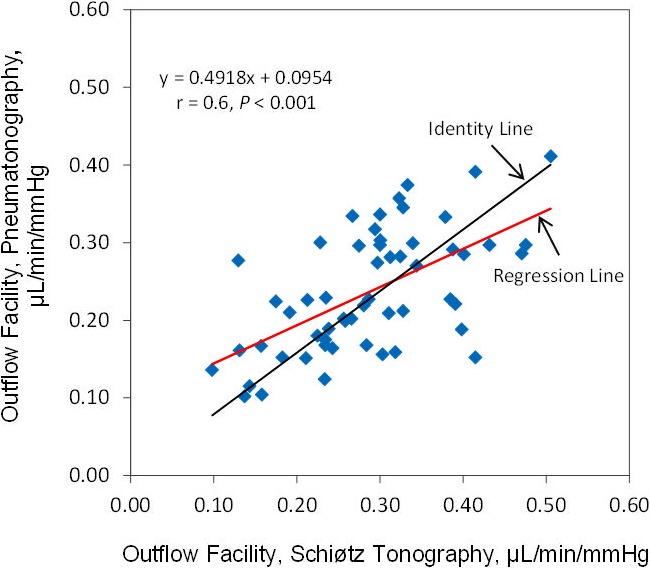
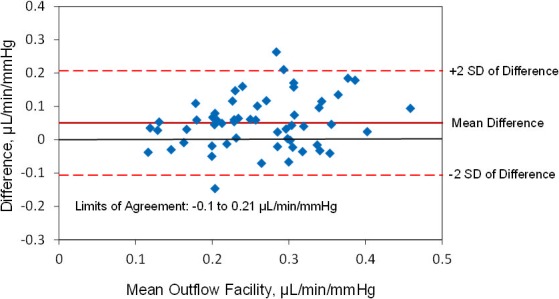
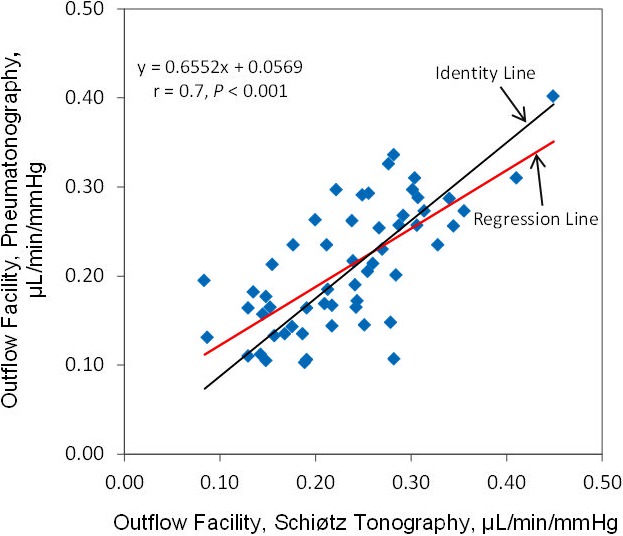
The outflow facility was 0.29 ± 0.09 μL/min/mm Hg by Schiøtz tonography and 0.24 ± 0.08 μL/min/mm Hg by pneumatonography (P < 0.001) when using the standard assumed constant ocular rigidity coefficient. Mean calculated ocular rigidity coefficient was 0.028 ± 0.01 μL-1, and outflow facility determined by using this coefficient was 0.23 ± 0.08 μL/min/mm Hg by Schiøtz tonography and 0.21 ± 0.07 μL/min/mm Hg by pneumatonography (P = 0.003). Outflow facilities measured by the two devices were correlated when the ocular rigidity was assumed (r = 0.60, P < 0.001) or calculated (r = 0.70, P < 0.001).
Outflow facilities measured by pneumatonography were correlated with those measured by Schiøtz tonography, but Schiøtz tonography reported approximately 10% to 20% higher facilities when using the standard method. When ocular rigidity was determined for each eye, differences were smaller. Measurements from these devices cannot be compared directly.
通过气动眼压描记法和施氏眼压计测量法测得的房水流出率是否可互换尚不清楚。在本研究中,我们比较了气动眼压描记法测得的房水流出率与数字式施氏眼压计测量法测得的房水流出率。
纳入28名年龄在41至68岁之间的健康参与者的56只眼睛。使用气动眼压计测量坐位和平卧位的眼压。受试者处于平卧位时,使用带有10克砝码的气动眼压计记录眼压2分钟,使用定制的数字式施氏眼压计记录眼压4分钟。分别根据压力和眼内体积的变化以及每种仪器的标准假定眼硬度系数,以及通过测量在气动眼压计尖端添加砝码前后的压力计算出的眼硬度系数来确定房水流出率。
使用标准假定恒定眼硬度系数时,施氏眼压计测量的房水流出率为0.29±0.09μL/min/mm Hg,气动眼压描记法测量的房水流出率为0.24±0.08μL/min/mm Hg(P<0.001)。平均计算眼硬度系数为0.028±0.01μL-1,使用该系数确定的房水流出率,施氏眼压计测量为0.23±0.08μL/min/mm Hg,气动眼压描记法测量为0.21±0.07μL/min/mm Hg(P=0.003)。当假定眼硬度(r=0.60,P<0.001)或计算眼硬度(r=0.70,P<0.001)时,两种设备测量的房水流出率具有相关性。
气动眼压描记法测量的房水流出率与施氏眼压计测量的房水流出率具有相关性,但使用标准方法时,施氏眼压计报告的房水流出率高出约10%至20%。当为每只眼睛确定眼硬度时,差异较小。这些设备的测量结果不能直接比较。