Acera Amelia, Manresa Josep Maria, Rodriguez Diego, Rodriguez Ana, Bonet Josep Maria, Trapero-Bertran Marta, Hidalgo Pablo, Sànchez Norman, de Sanjosé Silvia
Atenció a la Salut Sexual i Reproductiva (ASSIR) SAP Cerdanyola-Ripollet, Institut Català de la Salut, Ripollet, Spain.
Unitat de Suport a la Recerca Metropolitana Nord. Institut de Investigació en Atenció Primària (IDIAP) Jordi Gol. Sabadell, Spain.
PLoS One. 2017 Jan 24;12(1):e0170371. doi: 10.1371/journal.pone.0170371. eCollection 2017.
Opportunistic cervical cancer screening can lead to suboptimal screening coverage. Coverage could be increased after a personalised invitation to the target population. We present a community randomized intervention study with three strategies aiming to increase screening coverage.
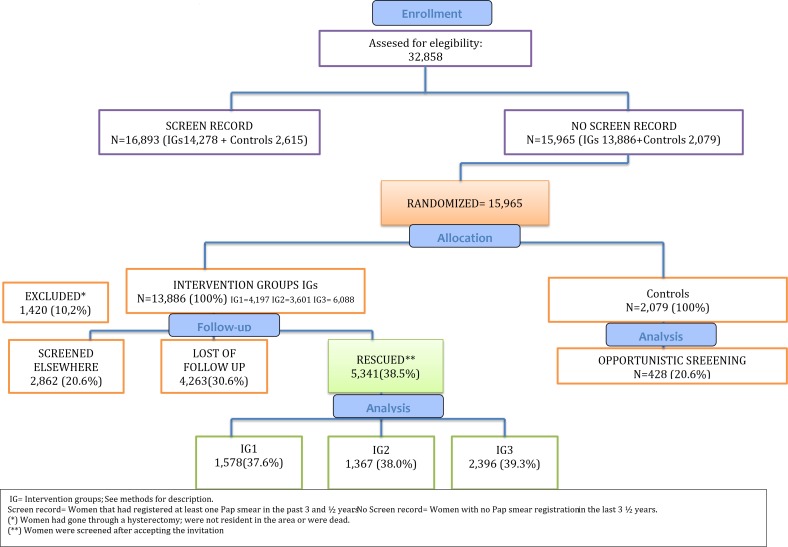
The CRICERVA study is a community-based clinical trial to improve coverage of population-based screening in the Cerdanyola SAP area in Barcelona.A total of 32,858 women residing in the study area, aged 30 to 70 years were evaluated. A total of 15,965 women were identified as having no registration of a cervical cytology in the last 3.5 years within the Public Health data base system. Eligible women were assigned to one of four community randomized intervention groups (IGs): (1) (IG1 N = 4197) personalised invitation letter, (2) (IG2 N = 3601) personalised invitation letter + informative leaflet, (3) (IG3 N = 6088) personalised invitation letter + informative leaflet + personalised phone call and (4) (Control N = 2079) based on spontaneous demand of cervical cancer screening as officially recommended. To evaluate screening coverage, we used heterogeneity tests to compare impact of the interventions and mixed logistic regression models to assess the age effect. We refer a "rescue" visit as the screening visit resulting from the study invitation.
Among the 13,886 women in the IGs, 2,862 were evaluated as having an adequate screening history after the initial contact; 4,263 were lost to follow-up and 5,341 were identified as having insufficient screening and thus being eligible for a rescue visit. All intervention strategies significantly increased participation to screening compared to the control group. Coverage after the intervention reached 84.1% while the control group reached 64.8%. The final impact of our study was an increase of 20% in the three IGs and of 9% in the control group (p<0.001). Within the intervention arms, age was an important determinant of rescue visits showing a statistical interaction with the coverage attained in the IGs. Within the intervention groups, final screening coverage was significantly higher in IG3 (84.4%) (p<0.001). However, the differences were more substantial in the age groups 50-59 and those 60+. The highest impact of the IG3 intervention was observed among women 60+ y.o with 32.0% of them being rescued for screening. The lowest impact of the interventions was in younger women.
The study confirms that using individual contact methods and assigning a fixed screening date notably increases participation in screening. The response to the invitation is strongly dependent on age.
ClinicalTrials.gov NCT01373723.
机会性宫颈癌筛查可能导致筛查覆盖率不理想。向目标人群发出个性化邀请后,覆盖率可能会提高。我们开展了一项社区随机干预研究,采用三种策略旨在提高筛查覆盖率。
CRICERVA研究是一项基于社区的临床试验,旨在提高巴塞罗那塞尔达尼奥拉卫生区人群筛查的覆盖率。对居住在研究区域内年龄在30至70岁的32,858名女性进行了评估。在公共卫生数据库系统中,共有15,965名女性被确定在过去3.5年内没有宫颈细胞学检查记录。符合条件的女性被分配到四个社区随机干预组之一:(1)(IG1,N = 4197)个性化邀请信;(2)(IG2,N = 3601)个性化邀请信 + 信息传单;(3)(IG3,N = 6088)个性化邀请信 + 信息传单 + 个性化电话;(4)(对照组,N = 2079)基于官方推荐的宫颈癌筛查自发需求。为了评估筛查覆盖率,我们使用异质性检验来比较干预措施的影响,并使用混合逻辑回归模型来评估年龄效应。我们将“补救”就诊定义为由研究邀请导致的筛查就诊。
在干预组的13,886名女性中,2,862名在初次接触后被评估为有足够的筛查史;4,263名失访,5,341名被确定为筛查不足,因此有资格进行补救就诊。与对照组相比,所有干预策略均显著提高了筛查参与率。干预后的覆盖率达到84.1%,而对照组为64.8%。我们研究的最终影响是三个干预组提高了20%,对照组提高了9%(p<0.001)。在干预组中,年龄是补救就诊的重要决定因素,与干预组达到的覆盖率存在统计学交互作用。在干预组中,IG3的最终筛查覆盖率显著更高(84.4%)(p<0.001)。然而,在50 - 59岁年龄组和60岁以上年龄组中差异更为显著。在60岁以上女性中观察到IG3干预的影响最大,其中32.0%的女性因筛查而得到补救。干预对年轻女性的影响最小。
该研究证实,采用个人联系方法并指定固定的筛查日期可显著提高筛查参与率。对邀请的响应强烈依赖于年龄。
ClinicalTrials.gov NCT01373723