Ustun C, Giannotti F, Zhang M-J, Wang H-L, Brunstein C, Labopin M, Rocha V, de Lima M, Baron F, Sandmaier B M, Eapen M, Gluckman E, Nagler A, Weisdorf D J, Ruggeri A
Division of Hematology, Oncology and Transplantation, Department of Medicine, University of Minnesota Medical Center, Minneapolis, MN, USA.
Service d'Hématologie et Thérapie Cellulaire, Hôpital Saint Antoine, AP-HP, Paris, France.
Leukemia. 2017 Jun;31(6):1408-1414. doi: 10.1038/leu.2017.42. Epub 2017 Jan 25.
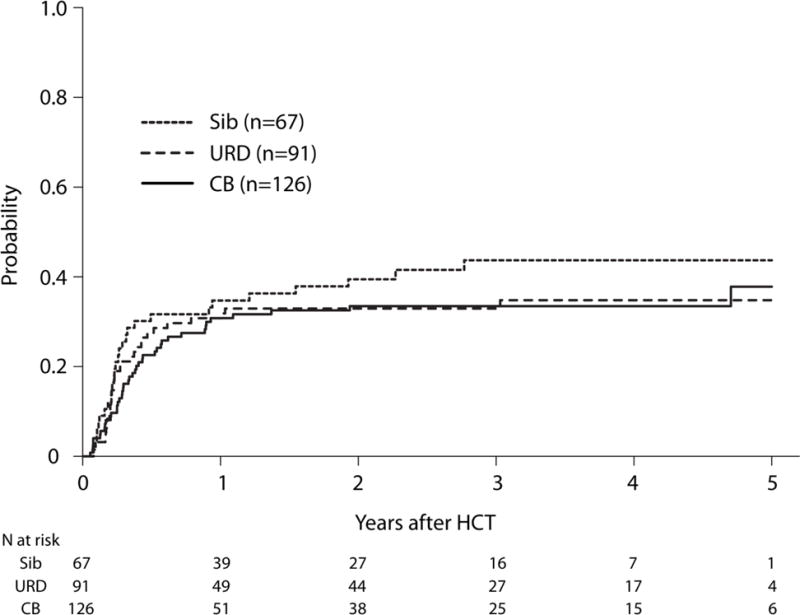
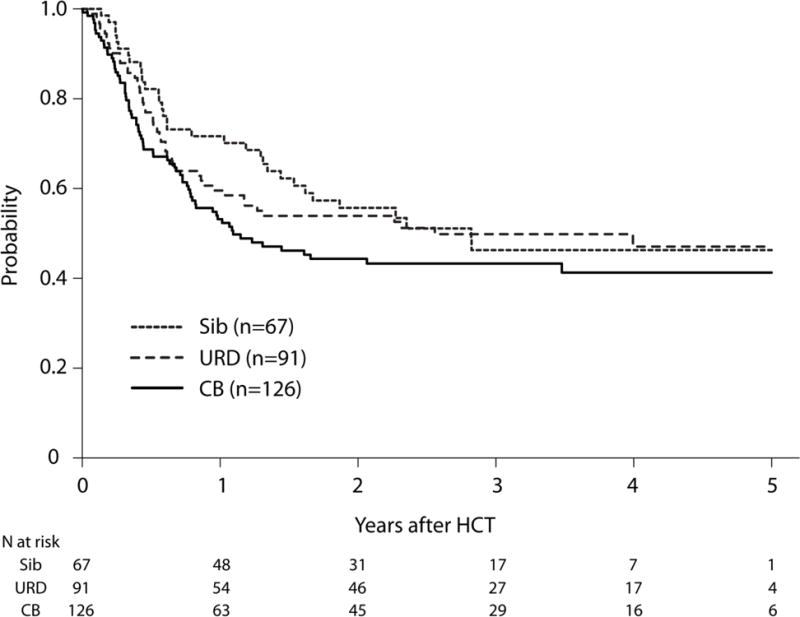
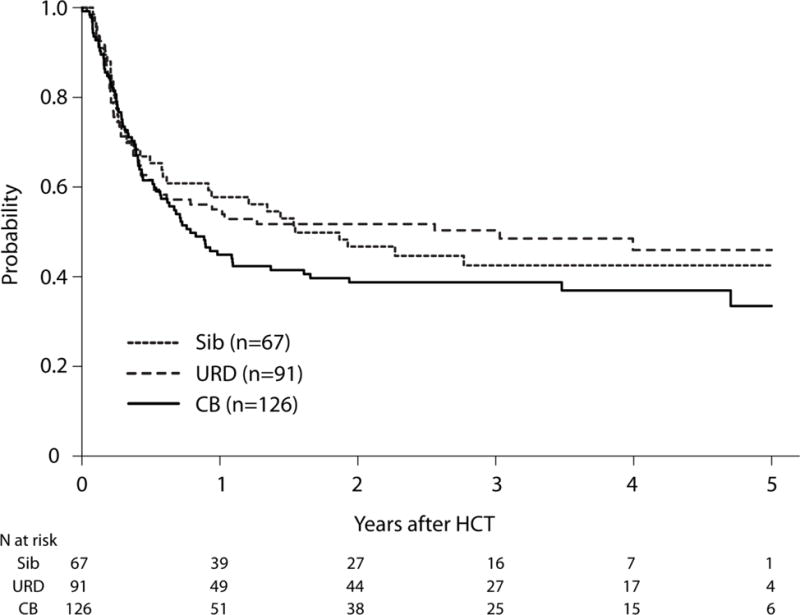
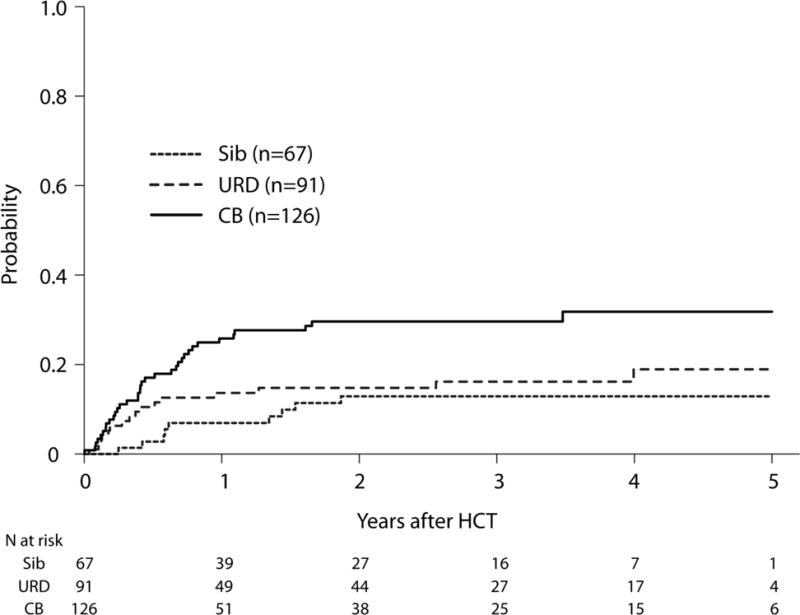
Allogeneic hematopoietic cell transplantation (HCT) from siblings or unrelated donors (URD) during complete remission (CR) may improve leukemia-free survival (LFS) in FMS-like tyrosine kinase 3+ (FLT3+) acute myeloid leukemia (AML), which has poor prognosis because of high relapse rates. Umbilical cord blood (UCB) HCT outcomes are largely unknown in this population. We found that compared with sibling HCT, relapse risks were similar after UCB (n=126) (hazard ratio (HR) 0.86, P=0.54) and URD (n=91) (HR 0.81, P=0.43). UCB HCT was associated with statistically higher non-relapse mortality compared with sibling HCT (HR 2.32, P=0.02), but not vs URD (HR 1.72, P=0.07). All three cohorts had statistically nonsignificant 3-year LFS: 39% (95% confidence interval (CI): 30-47) after UCB, 43% (95% CI: 30-54) after sibling and 50% (95% CI: 40-60) after URD. Chronic graft-versus-host disease rates were significantly lower after UCB compared with either sibling (HR 0.59, P=0.03) or URD (HR 0.49, P=0.001). Adverse factors for LFS included high leukocyte count at diagnosis and HCT during CR2 (second CR). UCB is a suitable option for adults with FLT3+ AML in the absence of an human leukocyte antigen-matched sibling and its immediate availability may be particularly important for FLT3+ AML where early relapse is common, thus allowing HCT in CR1 (first CR) when outcomes are best.
在完全缓解(CR)期间,来自同胞或无关供者(URD)的异基因造血细胞移植(HCT)可能会改善FMS样酪氨酸激酶3阳性(FLT3+)急性髓系白血病(AML)的无白血病生存期(LFS),该病因复发率高而预后较差。在这一人群中,脐带血(UCB)HCT的结果在很大程度上尚不清楚。我们发现,与同胞HCT相比,UCB(n = 126)移植后的复发风险相似(风险比[HR] 0.86,P = 0.54),URD(n = 91)移植后的复发风险也相似(HR 0.81,P = 0.43)。与同胞HCT相比,UCB HCT的非复发死亡率在统计学上更高(HR 2.32,P = 0.02),但与URD相比则不然(HR 1.72,P = 0.07)。所有三个队列的3年LFS在统计学上均无显著差异:UCB移植后为39%(95%置信区间[CI]:30 - 47),同胞移植后为43%(95% CI:30 - 54),URD移植后为50%(95% CI:40 - 60)。与同胞(HR 0.59,P = 0.03)或URD(HR 0.49,P = 0.001)相比,UCB移植后的慢性移植物抗宿主病发生率显著更低。LFS的不良因素包括诊断时白细胞计数高以及在第二次完全缓解(CR2)期间进行HCT。在没有人类白细胞抗原匹配同胞的情况下,UCB是FLT3+ AML成年患者的一个合适选择,其即时可用性对于FLT3+ AML可能尤为重要,因为早期复发很常见,从而允许在缓解效果最佳的第一次完全缓解(CR1)时进行HCT。