Kweon Sehi, Koo Bon Seok, Jee Sungju
Department of Rehabilitation Medicine, Chungnam National University Hospital, Daejeon, Korea.
Department of Otolaryngology-Head and Neck Surgery, Chungnam National University Hospital, Daejeon, Korea.
Ann Rehabil Med. 2016 Dec;40(6):1100-1107. doi: 10.5535/arm.2016.40.6.1100. Epub 2016 Dec 30.
To evaluate the functional characteristics of swallowing and to analyze the parameters of dysphagia in head and neck cancer patients after concurrent chemoradiotherapy (CCRT).
The medical records of 32 patients with head and neck cancer who were referred for a videofluoroscopic swallowing study from January 2012 to May 2015 were retrospectively reviewed. The patients were allocated by duration after starting CCRT into early phase (<1 month after radiation therapy) and late phase (>1 month after radiation therapy) groups. We measured the modified penetration aspiration scale (MPAS) and American Speech-Language-Hearing Association National Outcome Measurement System swallowing scale (ASHA-NOMS). The oral transit time (OTT), pharyngeal delay time (PDT), and pharyngeal transit time (PTT) were recorded to assess the swallowing physiology.
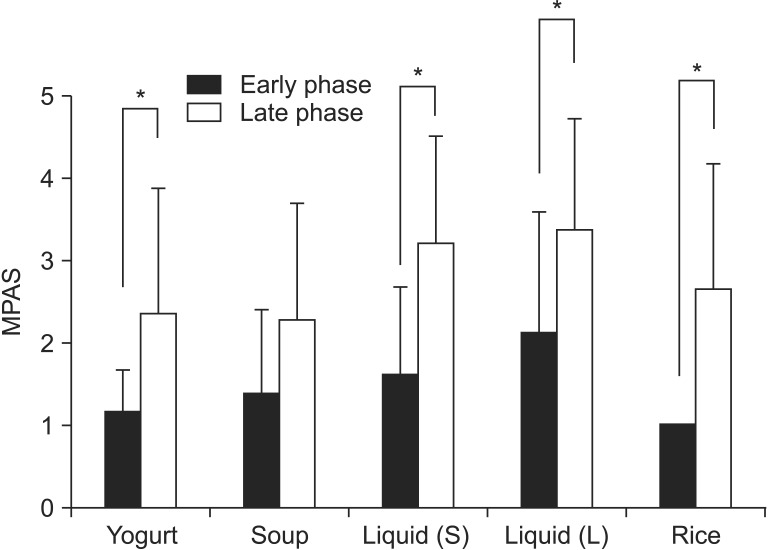
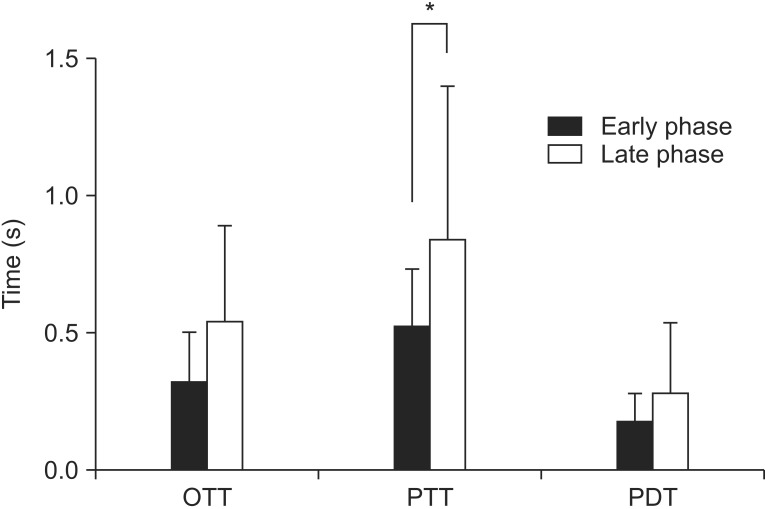
Among 32 cases, 18 cases (56%) were of the early phase. In both groups, the most common tumor site was the hypopharynx (43.75%) with a histologic type of squamous cell carcinoma (75%). PTT was significantly longer in the late phase (p=0.03). With all types of boluses, except for soup, both phases showed a statistically significant difference in MPAS results. The mean ASHA-NOMS level for the early phase was 5.83±0.78 and that for the late phase was 3.79±1.80, with statistical significance (p=0.01). The PTT and ASHA-NOMS level showed a statistically significant correlation (correlation coefficient=-0.52, p=0.02). However, it showed no relationship with the MPAS results.
The results of our study suggest that in the late phase that after CCRT, the OTT, PDT, and PTT were longer than in the early phase and the PTT prolongation was statistically significant. Therefore, swallowing therapy targeting the pharyngeal phase is recommended after CCRT.
评估头颈部癌患者同步放化疗(CCRT)后吞咽功能特征并分析吞咽困难参数。
回顾性分析2012年1月至2015年5月因视频荧光吞咽造影检查而转诊的32例头颈部癌患者的病历。根据开始CCRT后的持续时间将患者分为早期(放疗后<1个月)和晚期(放疗后>1个月)组。我们测量了改良渗透误吸量表(MPAS)和美国言语语言听力协会国家结果测量系统吞咽量表(ASHA-NOMS)。记录口腔通过时间(OTT)、咽部延迟时间(PDT)和咽部通过时间(PTT)以评估吞咽生理功能。
32例患者中,18例(56%)为早期。两组中,最常见的肿瘤部位是下咽(43.75%),组织学类型为鳞状细胞癌(75%)。晚期PTT显著延长(p=0.03)。对于除汤以外的所有类型食团,两个阶段的MPAS结果均有统计学显著差异。早期的平均ASHA-NOMS水平为5.83±0.78,晚期为3.79±1.80,具有统计学显著性(p=0.01)。PTT与ASHA-NOMS水平呈统计学显著相关(相关系数=-0.52,p=0.02)。然而,它与MPAS结果无关。
我们的研究结果表明,CCRT后的晚期,OTT、PDT和PTT比早期更长,且PTT延长具有统计学显著性。因此,建议CCRT后针对咽部阶段进行吞咽治疗。