Sendagire Cornelius, Lipnick Michael S, Kizito Sam, Kruisselbrink Rebecca, Obua Daniel, Ejoku Joseph, Ssemogerere Lameck, Nakibuuka Jane, Kwizera Arthur
Department of Anesthesia and critical care,, Makerere University College of Health Sciences, P.O. Box 7072, Kampala, Uganda.
San Francisco General Hospital, University of California San Francisco, 1001 Potrero, 3C24, San Francisco, CA, 94110, USA.
BMC Anesthesiol. 2017 Jan 26;17(1):12. doi: 10.1186/s12871-017-0304-8.
Sub-Saharan Africa has a great burden of critical illness with limited health care resources. We evaluated the feasibility and utility of the modified Sequential Organ Function Assessment (mSOFA) score in assessing morbidity and mortality in the National Referral Hospital's intensive care unit (ICU) for one year.
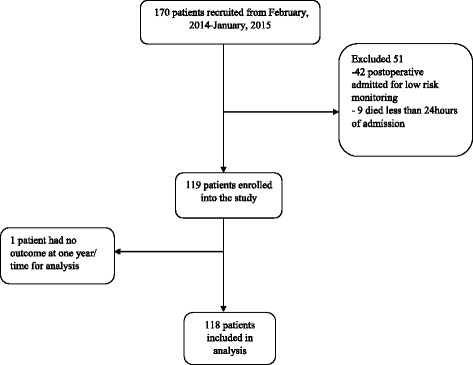
We conducted a prospective, observational cohort study on patients above 12 years of age admitted to the ICU at Mulago Hospital (Kampala, Uganda). All SOFA scores were determined at admission and at 48 h. We modified the SOFA score by replacing the PaO/FiO ratio with SPO/FiO. The primary outcome was ICU mortality.
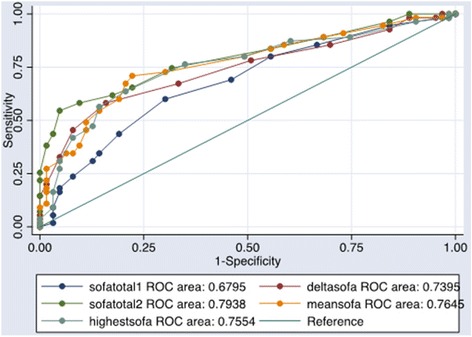
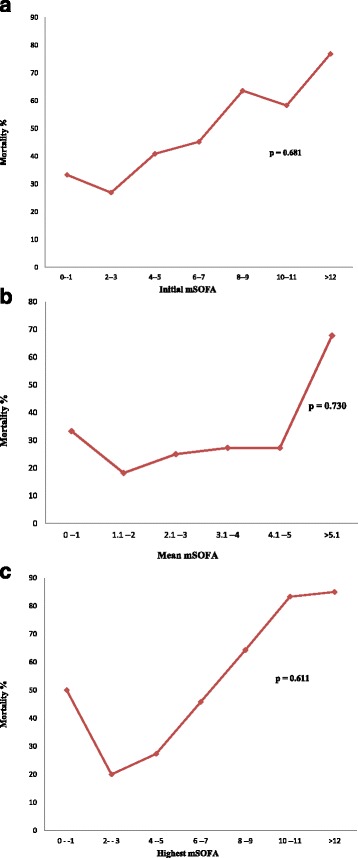
This ICU cohort of 118 patients had a mean age of 37 years and an ICU mortality rate of 46.6%. Non-survivors had higher initial (7.7 SD 3.8 vs. 5.5 SD 3.3; p = 0.007), mean (8.1 SD 3.9 vs 4.7 SD 2.6; p < 0.001) and highest mSOFA scores (9.4 SD 4.2 vs. 5.8 SD 3.2; p < 0.001), with an increase of 1.0 (SD 3.1) mSOFA on average after 48 h when compared to survivors (p < 0.001). The area under the receiver operating characteristic curves for each mSOFA category was: initial-0.68, mean-0.76, highest-0.76 and delta mSOFA-0.74. Multivariate logistic regression analysis showed no significant association between mSOFA scores and mortality.
Our results confirm that calculation of the mSOFA score is feasible for an ICU population in a resource-limited country. More data are needed to test for an association between mSOFA and mortality.
撒哈拉以南非洲地区面临着重大疾病负担,且卫生保健资源有限。我们评估了改良序贯器官功能评估(mSOFA)评分在一家国家级转诊医院重症监护病房(ICU)评估发病率和死亡率方面的可行性及实用性,为期一年。
我们对穆拉戈医院(乌干达坎帕拉)ICU收治的12岁以上患者进行了一项前瞻性观察性队列研究。所有SOFA评分均在入院时及48小时时测定。我们通过用SPO/FiO替代PaO/FiO比值来改良SOFA评分。主要结局为ICU死亡率。
该ICU队列中的118名患者平均年龄为37岁,ICU死亡率为46.6%。非幸存者的初始(7.7±3.8 vs. 5.5±3.3;p = 0.007)、平均(8.1±3.9 vs 4.7±2.6;p < 0.001)和最高mSOFA评分更高(9.4±4.2 vs. 5.8±3.2;p < 0.001),与幸存者相比,48小时后平均mSOFA增加1.0(±3.1)(p < 0.001)。每个mSOFA类别在受试者工作特征曲线下的面积分别为:初始-0.68、平均-0.76、最高-0.76和mSOFA差值-0.74。多因素逻辑回归分析显示mSOFA评分与死亡率之间无显著关联。
我们的结果证实,对于资源有限国家的ICU人群,计算mSOFA评分是可行的。需要更多数据来检验mSOFA与死亡率之间的关联。