Angelieri Fernanda, Franchi Lorenzo, Cevidanes Lucia H S, Bueno-Silva Bruno, McNamara James A
Assistant Professor, Guarulhos University, Guarulhos, Brazil; and Visiting Scholar, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, The University of Michigan, Ann Arbor, MI.
Research Associate, Department of Surgery and Translational Medicine, The University of Florence, Florence, Italy; and Thomas M. Graber Visiting Scholar, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, The University of Michigan, Ann Arbor, MI.
Dental Press J Orthod. 2016 Nov-Dec;21(6):115-125. doi: 10.1590/2177-6709.21.6.115-125.sar.
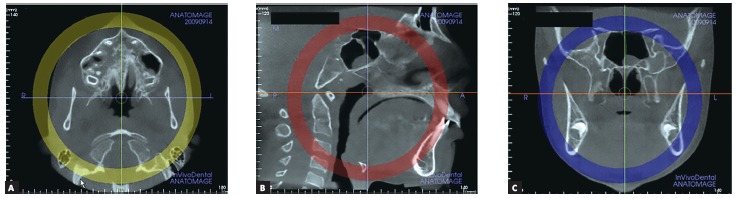
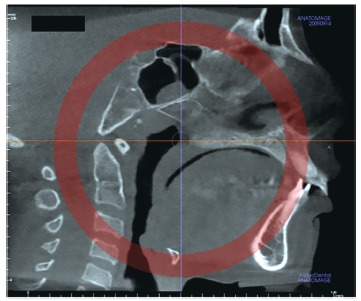
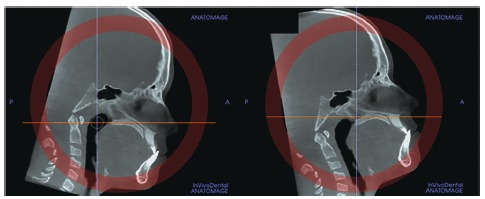
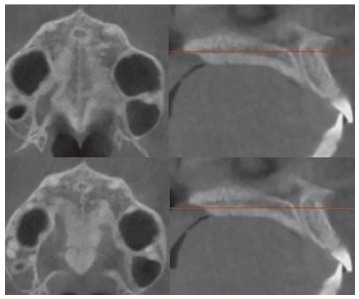
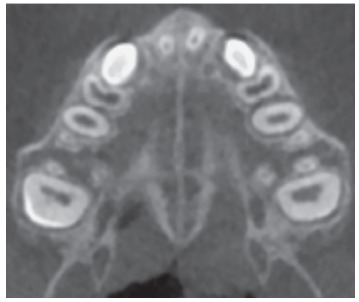
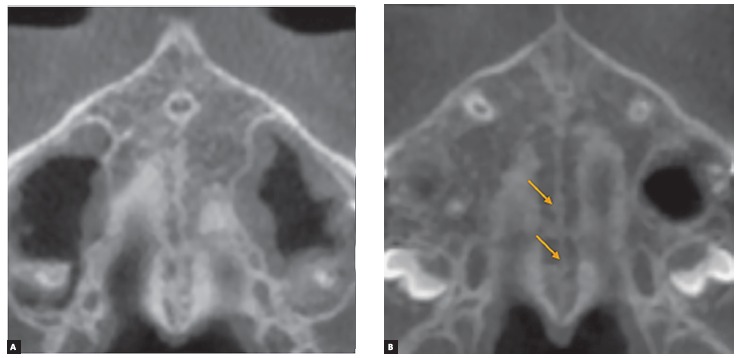
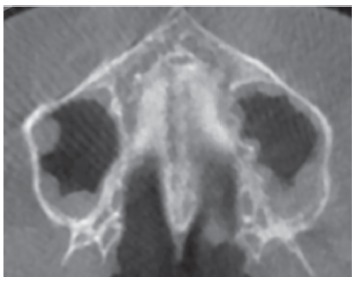
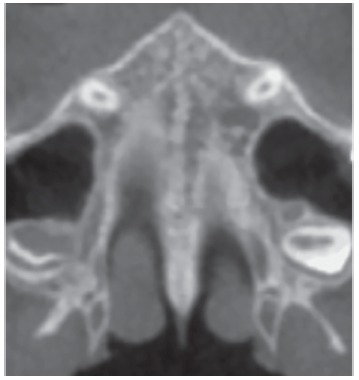
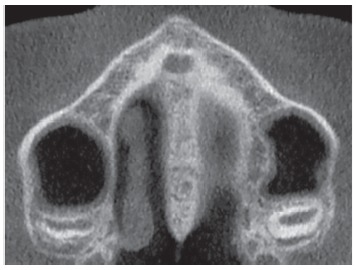
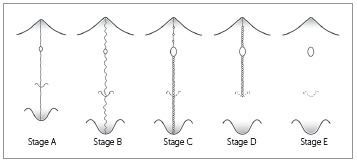
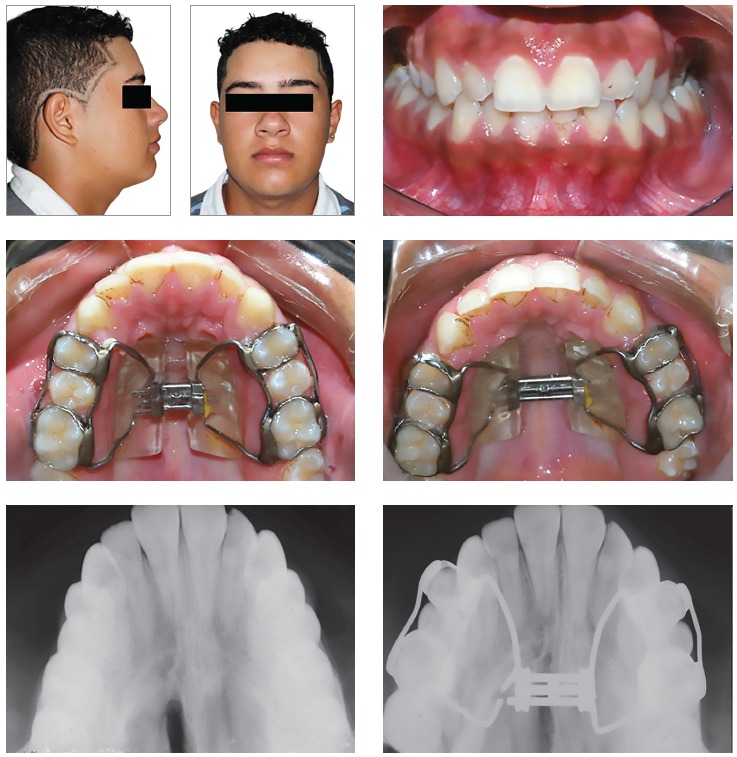
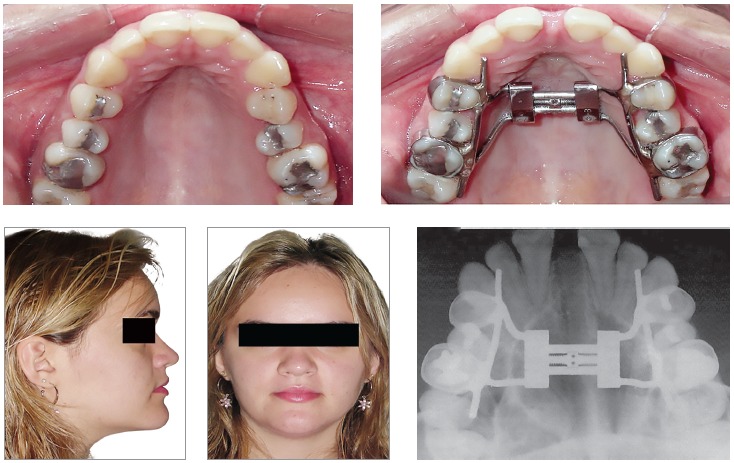
Rapid maxillary expansion (RME) primarily involves the mechanical opening of the midpalatal suture of the maxillary and palatine bones. The fusion of the midpalatal suture determines the failure of RME, a common event in late adolescents and young adults. Recently, the assessment of the maturation of midpalatal suture as viewed using cone beam computed tomography (CBCT) has been introduced. Five maturational stages of the midpalatal suture have been presented: Stage A = straight high-density sutural line, with no or little interdigitation; Stage B = scalloped appearance of the high-density sutural line; Stage C = two parallel, scalloped, high-density lines that lie close to each other, separated in some areas by small low-density spaces; Stage D = fusion of the palatine bone where no evidence of a suture is present; and Stage E = complete fusion that extends also anteriorly in the maxilla. At Stage C, less skeletal response would be expected than at Stages A and B, as there are many bony bridges along the suture. For patients at Stages D and E, surgically assisted RME would be necessary, as the fusion of the midpalatal suture already has occurred either partially or totally. This diagnostic method can be used to estimate the prognosis of the RME, mainly for late adolescents and young adults for whom this procedure is unpredictable clinically.
快速上颌扩弓(RME)主要涉及上颌骨和腭骨的腭中缝机械性打开。腭中缝融合决定了RME的失败,这在青少年晚期和年轻成年人中是常见情况。最近,引入了使用锥形束计算机断层扫描(CBCT)观察腭中缝成熟度的评估方法。腭中缝呈现出五个成熟阶段:A阶段 = 高密度的笔直缝线,无或仅有少量相互交错;B阶段 = 高密度缝线呈扇形外观;C阶段 = 两条平行、呈扇形的高密度线彼此靠近,在某些区域被小的低密度间隙分隔;D阶段 = 腭骨融合,无缝线迹象;E阶段 = 完全融合,且向前延伸至上颌骨。在C阶段,预计骨骼反应比A和B阶段少,因为沿缝线有许多骨桥。对于处于D和E阶段的患者,手术辅助RME是必要的,因为腭中缝已经部分或完全融合。这种诊断方法可用于估计RME的预后,主要针对青少年晚期和年轻成年人,该手术在临床上对他们来说是不可预测的。