Bodewes Thomas C F, Soden Peter A, Ultee Klaas H J, Zettervall Sara L, Pothof Alexander B, Deery Sarah E, Moll Frans L, Schermerhorn Marc L
Division of Vascular and Endovascular Surgery, Department of Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Mass; Department of Vascular Surgery, University Medical Center, Utrecht, The Netherlands.
Division of Vascular and Endovascular Surgery, Department of Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Mass.
J Vasc Surg. 2017 Feb;65(2):484-494.e3. doi: 10.1016/j.jvs.2016.08.093.
Unplanned hospital readmissions following surgical interventions are associated with adverse events and contribute to increasing health care costs. Despite numerous studies defining risk factors following lower extremity bypass surgery, evidence regarding readmission after endovascular interventions is limited. This study aimed to identify predictors of 30-day unplanned readmission following infrainguinal endovascular interventions.
We identified all patients undergoing an infrainguinal endovascular intervention in the targeted vascular module of the American College of Surgeons National Surgical Quality Improvement Program between 2012 and 2014. Perioperative outcomes were stratified by symptom status (chronic limb-threatening ischemia [CLI] vs claudication). Patients who died during index admission and those who remained in the hospital after 30 days were excluded. Indications for unplanned readmission related to the index procedure were evaluated. Multivariable logistic regression was used to identify preoperative and in-hospital (during index admission) risk factors of 30-day unplanned readmission.
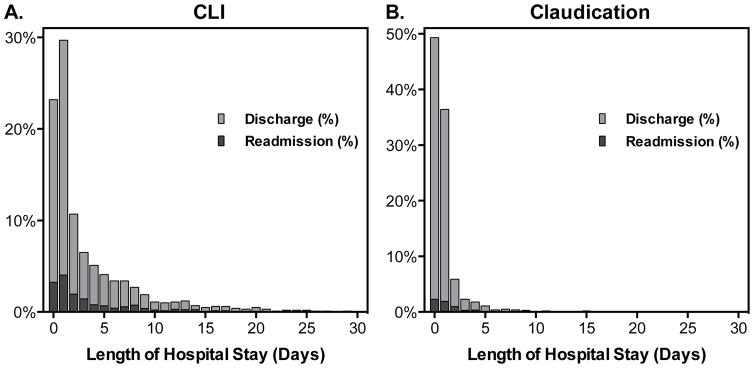
There were 4449 patients who underwent infrainguinal endovascular intervention, of whom 2802 (63%) had CLI (66% tissue loss) and 1647 (37%) had claudication. The unplanned readmission rates for CLI and claudication patients were 16% (n = 447) and 6.5% (n = 107), respectively. Mortality after index admission was higher for readmitted patients compared with those not readmitted (CLI, 3.4% vs 0.7% [P < .001]; claudication, 2.8% vs 0.1% [P < .01]). Approximately 50% of all unplanned readmissions were related to the index procedure. Among CLI patients, the most common indication for readmission related to the index procedure was wound or infection related (42%), whereas patients with claudication were mainly readmitted for recurrent symptoms of peripheral vascular disease (28%). In patients with CLI, predictors of unplanned readmission included diabetes (odds ratio, 1.3; 95% confidence interval, 1.01-1.6), congestive heart failure (1.6; 1.1-2.5), renal insufficiency (1.7; 1.3-2.2), preoperative dialysis (1.4; 1.02-1.9), tibial angioplasty/stenting (1.3; 1.04-1.6), in-hospital bleeding (1.9; 1.04-3.5), in-hospital unplanned return to the operating room (1.9; 1.1-3.5), and discharge other than to home (1.5; 1.1-2.0). Risk factors for those with claudication were dependent functional status (3.5; 1.4-8.7), smoking (1.6; 1.02-2.5), diabetes (1.5; 1.01-2.3), preoperative dialysis (3.6; 1.6-8.3), procedure time exceeding 120 minutes (1.8; 1.1-2.7), in-hospital bleeding (2.9; 1.2-7.4), and in-hospital unplanned return to the operating room (3.4; 1.2-9.4).
Unplanned readmission after endovascular treatment is relatively common, especially in patients with CLI, and is associated with substantially increased mortality. Awareness of these risk factors will help providers identify patients at high risk who may benefit from early surveillance, and prophylactic measures focused on decreasing postoperative complications may reduce the rate of readmission.
手术干预后的非计划住院再入院与不良事件相关,并导致医疗保健成本增加。尽管有大量研究确定了下肢搭桥手术后的风险因素,但关于血管内介入治疗后再入院的证据有限。本研究旨在确定腹股沟下血管内介入治疗后30天非计划再入院的预测因素。
我们确定了2012年至2014年期间在美国外科医师学会国家外科质量改进计划的目标血管模块中接受腹股沟下血管内介入治疗的所有患者。围手术期结果按症状状态(慢性肢体威胁性缺血[CLI]与间歇性跛行)分层。排除在首次入院期间死亡的患者和30天后仍住院的患者。评估与首次手术相关的非计划再入院的指征。使用多变量逻辑回归来确定30天非计划再入院的术前和住院期间(首次入院期间)风险因素。
共有4449例患者接受了腹股沟下血管内介入治疗,其中2802例(63%)患有CLI(66%有组织损失),1647例(37%)患有间歇性跛行。CLI和间歇性跛行患者的非计划再入院率分别为16%(n = 447)和6.5%(n = 107)。与未再入院的患者相比,再入院患者首次入院后的死亡率更高(CLI,3.4%对0.7%[P <.001];间歇性跛行,2.8%对0.1%[P <.01])。所有非计划再入院中约50%与首次手术相关。在CLI患者中,与首次手术相关的再入院最常见的指征是伤口或感染相关(42%),而间歇性跛行患者主要因外周血管疾病的复发症状而再入院(28%)。在CLI患者中,非计划再入院的预测因素包括糖尿病(比值比,1.3;95%置信区间,1.01 - 1.6)、充血性心力衰竭(1.6;1.1 - 2.5)、肾功能不全(1.7;1.3 - 2.2)、术前透析(1.4;1.02 - 1.9)、胫骨血管成形术/支架置入术(1.3;1.04 - 1.6)、住院期间出血(1.9;1.04 - 3.5)、住院期间非计划返回手术室(1.9;1.1 - 3.5)以及出院时非回家(1.5;1.1 - 2.0)。间歇性跛行患者的风险因素包括依赖性功能状态(比值比,3.5;1.4 - 8.7)、吸烟(1.6;1.02 - 2.5)、糖尿病(1.5;1.01 - 2.3)、术前透析(3.6;1.6 - 8.3)、手术时间超过120分钟(1.8;1.1 - 2.7)、住院期间出血(2.9;1.2 - 7.4)以及住院期间非计划返回手术室(3.4;1.2 - 9.4)。
血管内治疗后的非计划再入院相对常见,尤其是在CLI患者中,并且与死亡率大幅增加相关。了解这些风险因素将有助于医疗服务提供者识别可能从早期监测中获益的高危患者,而专注于减少术后并发症的预防措施可能会降低再入院率。