Wang Alex Y, Chughtai Abrar A, Lui Kei, Sullivan Elizabeth A
Faculty of Health, University of Technology Sydney, PO Box 123, Broadway, NSW, 2007, Australia.
School of Public Health and Community Medicine, University of New South Wales, Sydney, NSW, 2031, Australia.
BMC Pregnancy Childbirth. 2017 Feb 2;17(1):50. doi: 10.1186/s12884-017-1235-6.
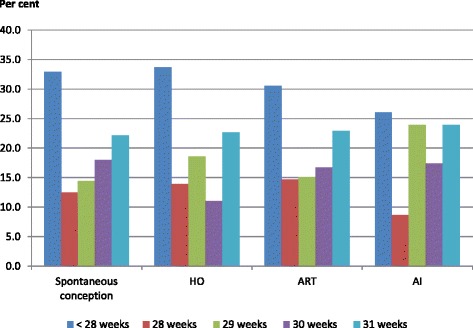
Due to high rates of multiple birth and preterm birth following fertility treatment, the rates of mortality and morbidity among births following fertility treatment were higher than those conceived spontaneously. However, it is unclear whether the rates of adverse neonatal outcomes remain higher for very preterm (<32 weeks gestational age) singletons born after fertility treatment. This study aims to compare adverse neonatal outcomes among very preterm singletons born after fertility treatment including assisted reproductive technology (ART) hyper-ovulution (HO) and artificial insemination (AI) to those following spontaneous conception.
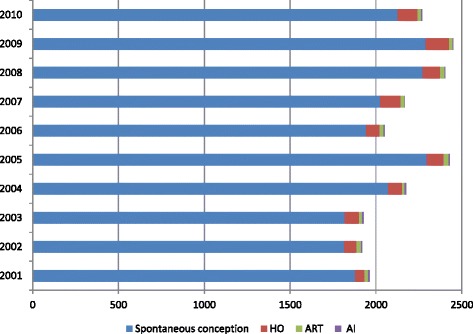
The population cohort study included 24069 liveborn very preterm singletons who were admitted to Neonatal Intensive Care Unit (NICU) in Australia and New Zealand from 2000 to 2010. The in-hospital neonatal mortality and morbidity among 21753 liveborn very preterm singletons were compared by maternal mode of conceptions: spontaneous conception, HO, ART and AI. Univariate and multivariate binary logistic regression analysis was used to examine the association between mode of conception and various outcome factors. Odds ratio (OR) and adjusted odds ratio (AOR) and 95% confidence interval (CI) were calculated.
The rate of small for gestational age was significantly higher in HO group (AOR 1.52, 95% CI 1.02-2.67) and AI group (AOR 2.98, 95% CI 1.53-5.81) than spontaneous group. The rate of birth defect was significantly higher in ART group (AOR 1.71, 95% CI 1.36-2.16) and AI group (AOR 3.01, 95% CI 1.47-6.19) compared to spontaneous group. Singletons following ART had 43% increased odds of necrotizing enterocolitis (AOR 1.43, 95% CI 1.04-1.97) and 71% increased odds of major surgery (AOR 1.71, 95% CI 1.37-2.13) compared to singletons conceived spontaneously. Other birth and NICU outcomes were not different among the comparison groups.
Compared to the spontaneous conception group, risk of congenital abnormality significantly increases after ART and AI; the risk of morbidities increases after ART, HO and AI. Preconception planning should include comprehensive information about the benefits and risks of fertility treatment on the neonatal outcomes.
由于生育治疗后多胎妊娠和早产的发生率较高,生育治疗后的出生死亡率和发病率高于自然受孕。然而,对于生育治疗后出生的极早产儿(孕周<32周)单胎,其不良新生儿结局的发生率是否仍然较高尚不清楚。本研究旨在比较生育治疗后出生的极早产单胎(包括辅助生殖技术(ART)、超促排卵(HO)和人工授精(AI))与自然受孕后的极早产单胎的不良新生儿结局。
这项人群队列研究纳入了2000年至2010年在澳大利亚和新西兰新生儿重症监护病房(NICU)住院的24069例极早产活产单胎。通过母亲受孕方式(自然受孕、HO、ART和AI)比较21753例极早产活产单胎的院内新生儿死亡率和发病率。采用单因素和多因素二元逻辑回归分析来检验受孕方式与各种结局因素之间的关联。计算优势比(OR)、调整优势比(AOR)和95%置信区间(CI)。
HO组(AOR 1.52,95% CI 1.02 - 2.67)和AI组(AOR 2.98,95% CI 1.53 - 5.81)小于胎龄儿的发生率显著高于自然受孕组。与自然受孕组相比,ART组(AOR 1.71,95% CI 1.36 - 2.16)和AI组(AOR 3.01,95% CI 1.47 - 6.19)出生缺陷的发生率显著更高。与自然受孕的单胎相比,ART后的单胎坏死性小肠结肠炎的发生几率增加43%(AOR 1.43,95% CI 1.04 - 1.97),大手术的发生几率增加71%(AOR 1.71,95% CI 1.37 - 2.13)。其他出生和NICU结局在各比较组之间无差异。
与自然受孕组相比,ART和AI后先天性异常的风险显著增加;ART、HO和AI后发病风险增加。孕前规划应包括关于生育治疗对新生儿结局的益处和风险的全面信息。