Mitchell Rebecca J, Cameron Cate M, McClure Rod
Australian Institute of Health Innovation, Macquarie University, Level 6, 75 Talavera Road, North Ryde, NSW, 2109, Australia.
Menzies Health Institute Queensland, Griffith University, Gold Coast, Australia.
BMC Public Health. 2017 Feb 2;17(1):150. doi: 10.1186/s12889-017-4087-0.
Improved understanding of long-term mortality attributable to injury is needed to accurately inform injury burden studies. This study aims to quantify and describe mortality attributable to injury 12 months after an injury-related hospitalisation in Australia.
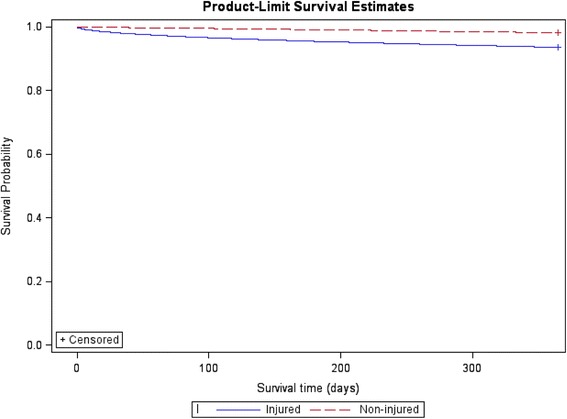
A population-based matched cohort study using linked hospital and mortality data from three Australian states during 2008-2010 was conducted. The injured cohort included individuals ≥18 years who had an injury-related hospital admission in 2009. A comparison cohort of non-injured people was obtain by randomly selecting from the electoral roll. This comparison group was matched 1:1 on age, gender and postcode of residence. Pre-index injury health service use and 12-month mortality were examined. Adjusted mortality rate ratios (MRR) and attributable risk were calculated. Cox proportional hazard regression was used to examine the effect of risk factors on survival.
Injured individuals were almost 3 times more likely to die within 12 months following an injury (MRR 2.90; 95% CI: 2.76-3.04). Individuals with a traumatic brain injury (MRR 7.58; 95% CI: 5.92-9.70) or injury to internal organs (MRR 7.38; 95% CI: 5.90-9.22) were 7 times more likely to die than the non-injured group. Injury was likely to be a contributory factor in 92% of mortality within 30 days and 66% of mortality at 12 months following the index injury hospital admission. Adjusted mortality rate ratios varied by type of cause-specific death, with MRR highest for injury-related deaths.
There are likely chronic consequences of sustaining a traumatic injury. Longer follow-up post-discharge is needed to consider deaths likely to be attributable to the injury. Better enumeration of long-term injury-related mortality will have the potential to improve estimates of injury burden.
为准确开展伤害负担研究,需要更深入了解伤害所致的长期死亡率。本研究旨在量化并描述澳大利亚因伤害相关住院治疗12个月后因伤害导致的死亡率。
采用基于人群的匹配队列研究,利用2008 - 2010年澳大利亚三个州的医院与死亡率关联数据。受伤队列包括2009年因伤害相关住院的18岁及以上个体。通过从选民名册中随机选取获得非受伤人群的对照队列。该对照组在年龄、性别和居住邮政编码方面按1:1进行匹配。检查指数伤害前的医疗服务使用情况和12个月死亡率。计算调整后的死亡率比值(MRR)和归因风险。采用Cox比例风险回归分析危险因素对生存的影响。
受伤个体在受伤后12个月内死亡的可能性几乎是非受伤个体的3倍(MRR 2.90;95%可信区间:2.76 - 3.04)。患有创伤性脑损伤(MRR 7.58;95%可信区间:5.92 - 9.70)或内脏损伤(MRR 7.38;95%可信区间:5.90 - 9.22)的个体死亡可能性是非受伤组的7倍。在指数伤害住院后30天内,92%的死亡中伤害可能是一个促成因素,在12个月时这一比例为66%。调整后的死亡率比值因死因特异性死亡类型而异,与伤害相关死亡的MRR最高。
遭受创伤性伤害可能存在慢性后果。出院后需要更长时间的随访以考虑可能归因于伤害的死亡。更好地统计与伤害相关的长期死亡率将有可能改进伤害负担的估计。