Westerik Janine A M, Metting Esther I, van Boven Job F M, Tiersma Waling, Kocks Janwillem W H, Schermer Tjard R
Department of Primary and Community Care, Radboud University Medical Center, 117-ELG, Geert Grooteplein Noord 21, Nijmegen, 6525 EZ, The Netherlands.
Department of General Practice, Groningen Research Institute for Asthma and COPD (GRIAC), University Medical Center Groningen, University of Groningen, HPC FA21, Antonius Deusinglaan 1, Groningen, 9713 AV, The Netherlands.
Respir Res. 2017 Feb 6;18(1):31. doi: 10.1186/s12931-017-0512-2.
COPD often coexists with chronic conditions that may influence disease prognosis. We investigated associations between chronic (co)morbidities and exacerbations in primary care COPD patients.
Retrospective cohort study based on 2012-2013 electronic health records from 179 Dutch general practices. Comorbidities from patients with physician-diagnosed COPD were categorized according to International Classification of Primary Care (ICPC) codes. Chi-squared tests, uni- and multivariable logistic, and Cox regression analyses were used to study associations with exacerbations, defined as oral corticosteroid prescriptions.
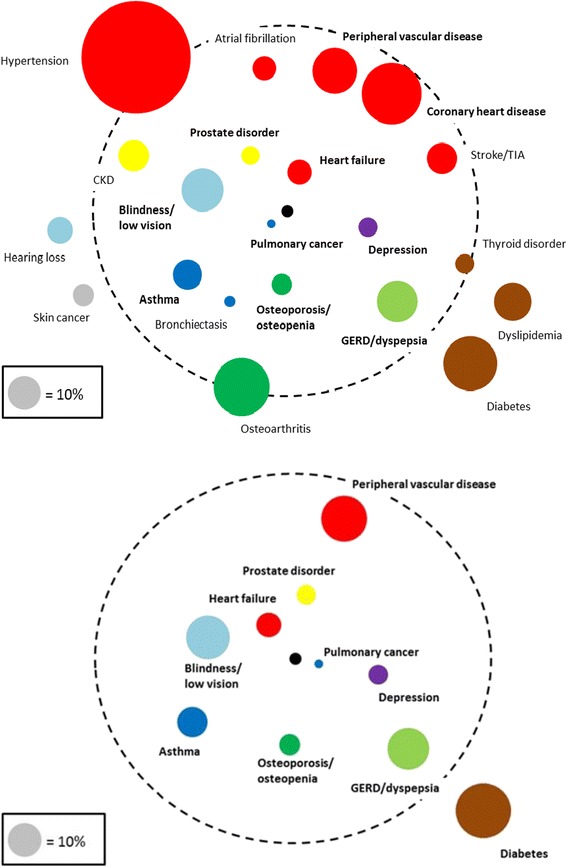
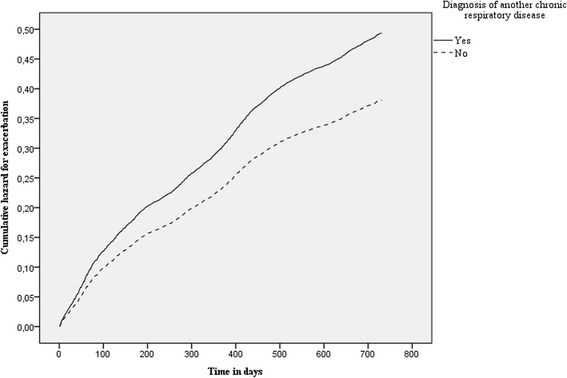
Fourteen thousand six hundred three patients with COPD could be studied (mean age 67 (SD 12) years, 53% male) for two years. At baseline 12,826 (88%) suffered from ≥1 comorbidities, 3263 (22%) from ≥5. The most prevalent comorbidities were hypertension (35%), coronary heart disease (19%), and osteoarthritis (18%). Several comorbidities showed statistically significant associations with frequent (i.e., ≥2/year) exacerbations: heart failure (odds ratio [OR], 95% confidence interval: 1.72; 1.38-2.14), blindness & low vision (OR 1.46; 1.21-1.75), pulmonary cancer (OR 1.85; 1.28-2.67), depression 1.48; 1.14-1.91), prostate disorders (OR 1.50; 1.13-1.98), asthma (OR 1.36; 1.11-1.70), osteoporosis (OR 1.41; 1.11-1.80), diabetes (OR 0.80; 0.66-0.97), dyspepsia (OR 1.25; 1.03-1.50), and peripheral vascular disease (OR 1.20; 1.00-1.45). From all comorbidity categories, having another chronic respiratory disease beside COPD showed the highest risk for developing a new exacerbation (Cox hazard ratio 1.26; 1.17-1.36).
Chronic comorbidities are highly prevalent in primary care COPD patients. Several chronic comorbidities were associated with having frequent exacerbations and increased exacerbation risk.
慢性阻塞性肺疾病(COPD)常与可能影响疾病预后的慢性疾病共存。我们调查了基层医疗COPD患者慢性共病与急性加重之间的关联。
基于179家荷兰全科诊所2012 - 2013年电子健康记录的回顾性队列研究。根据国际初级保健分类(ICPC)编码对医生诊断为COPD患者的共病进行分类。采用卡方检验、单变量和多变量逻辑回归以及Cox回归分析来研究与急性加重的关联,急性加重定义为口服糖皮质激素处方。
对14603例COPD患者进行了为期两年的研究(平均年龄67岁(标准差12岁),53%为男性)。基线时,12826例(88%)患有≥1种共病,3263例(22%)患有≥5种共病。最常见的共病是高血压(35%)、冠心病(19%)和骨关节炎(18%)。几种共病与频繁(即≥2次/年)急性加重存在统计学显著关联:心力衰竭(比值比[OR],95%置信区间:1.72;1.38 - 2.14)、失明和视力低下(OR 1.46;1.21 - 1.75)、肺癌(OR 1.85;1.28 - 2.67)、抑郁症(OR 1.48;1.14 - 1.91)、前列腺疾病(OR 1.50;1.13 - 1.98)、哮喘(OR 1.36;1.11 - 1.70)、骨质疏松症(OR 1.41;1.11 - 1.80)、糖尿病(OR 0.80;0.66 - 0.97)、消化不良(OR 1.25;1.03 - 1.50)和外周血管疾病(OR 1.20;1.00 - 1.45)。在所有共病类别中,除COPD外患有另一种慢性呼吸道疾病发生新急性加重的风险最高(Cox风险比1.26;1.17 - 1.36)。
慢性共病在基层医疗COPD患者中非常普遍。几种慢性共病与频繁急性加重及急性加重风险增加相关。