DiPaolo Giovanni, Jimenez-Moreno Cecilia, Nikolenko Nikoletta, Atalaia Antonio, Monckton Darren G, Guglieri Michela, Lochmüller Hanns
Keel University School of Medicine, Stoke-on-Trent, UK.
John Walton Muscular Dystrophy Research Centre, Newcastle University, Newcastle upon Tyne, UK.
J Neurol. 2017 Apr;264(4):701-708. doi: 10.1007/s00415-017-8399-x. Epub 2017 Feb 6.
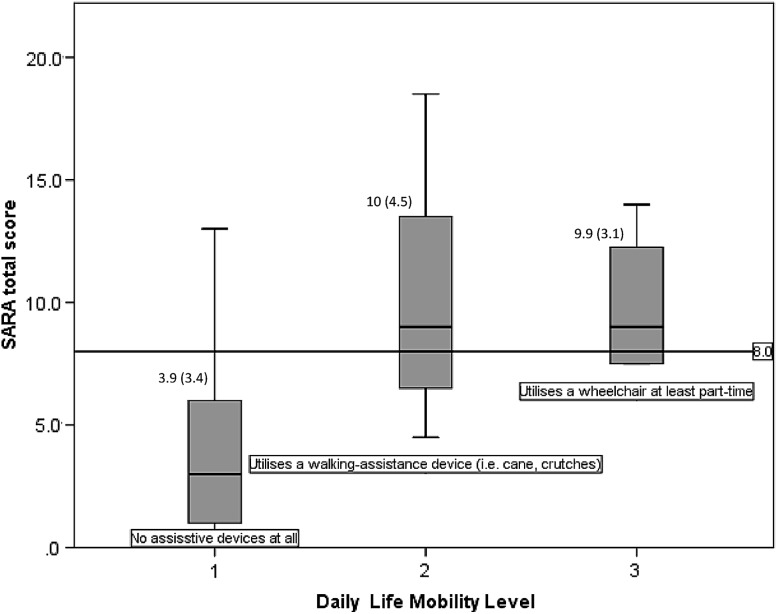
Myotonic dystrophy type 1 (DM1) is not characterised by ataxia per se; however, DM1 and ataxia patients show similar disturbances in movement coordination often experiencing walking and balance difficulties, although caused by different underlying pathologies. This study aims to investigate the use of a scale previously described for the assessment and rating of ataxia (SARA) with the hypothesis that it could have utility in DM1 patients as a measure of disease severity and risk of falling. Data from 54 DM1 patients were pulled from the PHENO-DM1 natural history study for analysis. Mean SARA score in the DM1 population was 5.45 relative to the maximum score of eight. A flooring effect (score 0) was observed in mild cases within the sample. Inter-rater and test-retest reliability was high with intraclass coefficients (ICC) of 0.983 and 1.00, respectively. Internal consistency was acceptable as indicated by a Cronbach's alpha of 0.761. Component analysis revealed two principle components. SARA correlated with: (1) all measures of muscle function tested, including quantitative muscle testing of ankle dorsiflexion (r = -0.584*), the 6 min walk test (r = -0.739*), 10 m walk test (r = 0.741*), and the nine hole peg test (r = 0.602*) and (2) measures of disease severity/burden, such as MIRS (r = 0.718*), MDHI (r = 0.483*), and DM1-Activ (r = -0.749*) (*p < 0.001). The SARA score was predicted by an interaction between modal CTG repeat length and age at sampling (r = 0.678, p = 0.003). A score of eight or above predicted the use of a walking aid with a sensitivity of 100% and a specificity of 85.7%. We suggest that further research is warranted to ascertain whether SARA or components of SARA are useful outcome measures for clinical trials in DM1. As a tool, it can be used for gathering information about disease severity/burden and helping to identify patients in need of a walking aid, and can potentially be applied in both research and healthcare settings.
1型强直性肌营养不良(DM1)本身并不以共济失调为特征;然而,DM1患者和共济失调患者在运动协调方面表现出相似的障碍,经常出现行走和平衡困难,尽管其潜在病因不同。本研究旨在调查一种先前描述的用于评估和分级共济失调的量表(SARA)的使用情况,假设它可用于DM1患者,作为疾病严重程度和跌倒风险的一种衡量指标。从PHENO-DM1自然史研究中提取了54例DM1患者的数据进行分析。DM1人群的SARA平均得分为5.45(满分8分)。在样本中的轻症病例中观察到地板效应(得分0)。评分者间信度和重测信度较高,组内相关系数(ICC)分别为0.983和1.00。Cronbach's α系数为0.761,表明内部一致性可接受。成分分析揭示了两个主要成分。SARA与以下因素相关:(1)所有测试的肌肉功能指标,包括踝背屈的定量肌肉测试(r = -0.584*)、6分钟步行试验(r = -0.739*)、10米步行试验(r = 0.741*)和九孔插板试验(r = 0.602*);(2)疾病严重程度/负担的指标,如MIRS(r = 0.718*)、MDHI(r = 0.483*)和DM1-Activ(r = -0.749*)(*p < 0.001)。SARA评分由采样时的模态CTG重复长度与年龄之间的相互作用预测(r = 0.678,p = 0.003)。8分及以上的评分预测使用助行器的敏感性为100%,特异性为85.7%。我们建议有必要进一步研究以确定SARA或SARA的组成部分是否是DM1临床试验有用的结局指标。作为一种工具,它可用于收集有关疾病严重程度/负担的信息,并有助于识别需要助行器的患者,并且有可能应用于研究和医疗保健环境。