Lin Jianqing, Patel Sheel A, Sama Ashwin R, Hoffman-Censits Jean H, Kennedy Brooke, Kilpatrick Deborah, Ye Zhong, Yang Hushan, Mu Zhaomei, Leiby Benjamin, Lewis Nancy, Cristofanilli Massimo, Kelly William Kevin
Thomas Jefferson University, Philadelphia, Pennsylvania, USA
George Washington University, Washington, D.C., USA.
Oncologist. 2016 Nov;21(11):1296-1297e. doi: 10.1634/theoncologist.2016-0297. Epub 2016 Oct 24.
Patients with metastatic castration-resistant prostate cancer did not tolerate the combination of alisertib with abiraterone and prednisone.There was no clear signal indicating that adding alisertib might be beneficial for those patients progressing on abiraterone.
We hypothesized that Aurora A kinase (AK) contributes to castrate resistance in prostate cancer (PCa) and that inhibiting AK with alisertib can resensitize PCa cells to androgen receptor (AR) inhibitor abiraterone.
This was a phase I/II trial to determine the safety and efficacy of alisertib when given in combination with abiraterone plus prednisone (AP). Metastatic castration-resistant prostate cancer (mCRPC) patients were treated with dose escalation (alisertib at 30, 40, and 50 mg orally b.i.d., days 1-7 every 21 days) per standard 3+3 design.
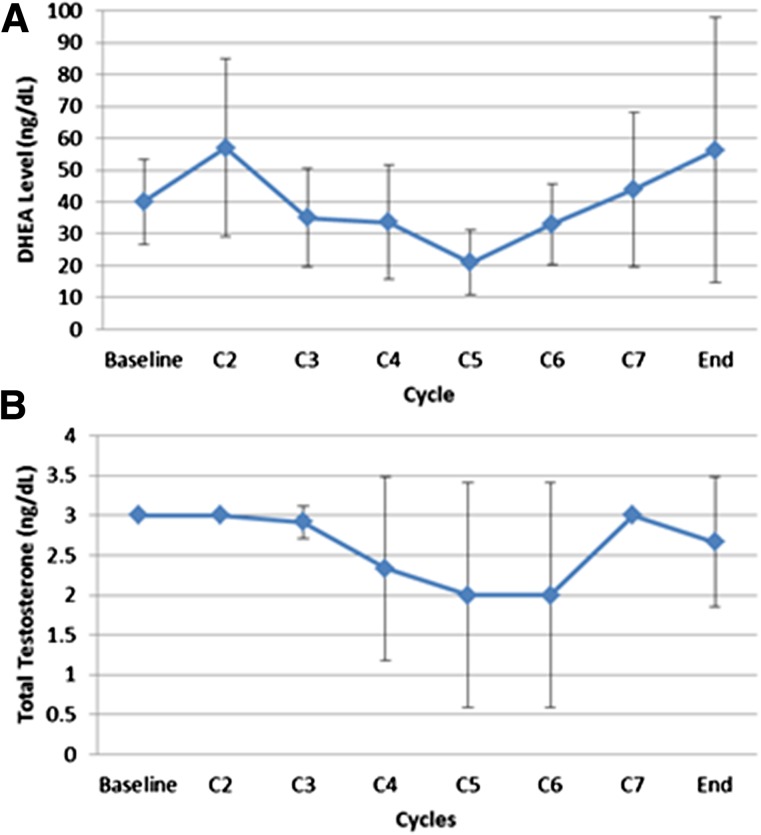
Nine of 43 planned subjects were enrolled. The maximum tolerated dose (MTD) was not reached, and the dose-limiting toxicities (DLTs) included neutropenic fever (1 of 9), neutropenia (1 of 9), fatigue with memory impairment (1 of 9), and diarrhea/mucositis (1 of 9). No prostate-specific antigen (PSA) decrease or circulating tumor cell (CTC) changes were observed during the study. Pharmacodynamically, adding alisertib did not affect total testosterone or dehydroepiandrosterone (DHEA) levels. There was some change in neuroendocrine markers after therapy. Mean duration on study was 2.5 months. The trial was terminated early.
A tolerable dose of alisertib in combination with AP in mCRPC was not established in this study. There was no clear signal indicating that alisertib might be beneficial for patients with mCRPC progressing on abiraterone.
转移性去势抵抗性前列腺癌患者无法耐受阿利塞替尼与阿比特龙和泼尼松的联合用药。没有明确迹象表明,对于在阿比特龙治疗期间病情进展的患者,添加阿利塞替尼可能有益。
我们假设极光激酶A(AK)在前列腺癌(PCa)的去势抵抗中起作用,并且用阿利塞替尼抑制AK可使PCa细胞对雄激素受体(AR)抑制剂阿比特龙重新敏感。
这是一项I/II期试验,旨在确定阿利塞替尼与阿比特龙加泼尼松(AP)联合使用时的安全性和有效性。转移性去势抵抗性前列腺癌(mCRPC)患者按照标准的3+3设计进行剂量递增治疗(阿利塞替尼口服,剂量为30、40和50mg,每日两次,第1-7天,每21天一个周期)。
计划入组的43名受试者中有9名入组。未达到最大耐受剂量(MTD),剂量限制毒性(DLT)包括中性粒细胞减少性发热(9例中的1例)、中性粒细胞减少(9例中的1例)、伴有记忆障碍的疲劳(9例中的1例)和腹泻/粘膜炎(9例中的1例)。在研究期间未观察到前列腺特异性抗原(PSA)降低或循环肿瘤细胞(CTC)变化。从药效学角度看,添加阿利塞替尼不影响总睾酮或脱氢表雄酮(DHEA)水平。治疗后神经内分泌标志物有一些变化。研究的平均持续时间为2.5个月。试验提前终止。
本研究未确定阿利塞替尼与AP联合用于mCRPC时的可耐受剂量。没有明确迹象表明,阿利塞替尼对在阿比特龙治疗期间病情进展的mCRPC患者可能有益。