Parikh Mamta, Liu Chengfei, Wu Chun-Yi, Evans Christopher P, Dall'Era Marc, Robles Daniel, Lara Primo N, Agarwal Neeraj, Gao Allen C, Pan Chong-Xian
Division of Hematology Oncology, Department of Internal Medicine, School of Medicine, University of California, Davis, USA.
Department of Urologic Surgery, School of Medicine, University of California, Davis, USA.
Sci Rep. 2021 Mar 18;11(1):6377. doi: 10.1038/s41598-021-85969-x.
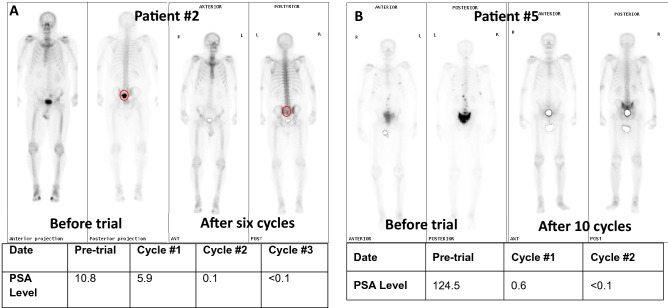
Niclosamide has preclinical activity against a wide range of cancers. In prostate cancer, it inhibits androgen receptor variant 7 and synergizes with abiraterone. The approved niclosamide formulation has poor oral bioavailability. The primary objective of this phase Ib trial was to identify a maximum tolerated dose (MTD) and recommended phase 2 dose (RP2D) of a novel reformulated orally-bioavailable niclosamide/PDMX1001 in combination with abiraterone and prednisone in men with castration-resistant prostate cancer (CRPC). Eligible patients had progressing CRPC, adequate end-organ function, and no prior treatment with abiraterone or ketoconazole. Patients were treated with escalating doses of niclosamide/PDMX1001 and standard doses of abiraterone and prednisone. Peak and trough niclosamide plasma levels were measured. Common Terminology Criteria for Adverse Events (CTCAE) v4.0 and Prostate Cancer Working Group 2 criteria were used to evaluate toxicities and responses. Nine patients with metastatic CRPC were accrued, with no dose-limiting toxicities observed at all dose levels. The recommended Phase II dose of niclosamide/PDMX1001 was 1200 mg orally (PO) three times daily plus abiraterone 1000 mg PO once daily and prednisone 5 mg PO twice daily. Trough and peak niclosamide concentrations exceeded the therapeutic threshold of > 0.2 µM. The combination was well tolerated with most frequent adverse effects of diarrhea. Five out of eight evaluable patients achieved a PSA response; two achieved undetectable PSA and radiographic response. A novel niclosamide/PDMX1001 reformulation achieved targeted plasma levels when combined with abiraterone and prednisone, and was well tolerated. Further study of niclosamide/PDMX1001 with this combination is warranted.
氯硝柳胺对多种癌症具有临床前活性。在前列腺癌中,它可抑制雄激素受体变体7,并与阿比特龙协同作用。已获批的氯硝柳胺制剂口服生物利用度较差。这项Ib期试验的主要目的是确定一种新型重新配方的口服生物利用度良好的氯硝柳胺/PDMX1001与阿比特龙和泼尼松联合用于去势抵抗性前列腺癌(CRPC)男性患者的最大耐受剂量(MTD)和推荐的2期剂量(RP2D)。符合条件的患者患有进展性CRPC,终末器官功能良好,且之前未接受过阿比特龙或酮康唑治疗。患者接受递增剂量的氯硝柳胺/PDMX1001以及标准剂量的阿比特龙和泼尼松治疗。测量了氯硝柳胺的血浆峰浓度和谷浓度。采用不良事件通用术语标准(CTCAE)v4.0和前列腺癌工作组2标准来评估毒性和反应。招募了9名转移性CRPC患者,在所有剂量水平均未观察到剂量限制性毒性。氯硝柳胺/PDMX1001的推荐II期剂量为口服(PO)1200毫克,每日三次,加阿比特龙1000毫克,每日一次口服,泼尼松5毫克,每日两次口服。氯硝柳胺的谷浓度和峰浓度超过了>0.2微摩尔的治疗阈值。该联合用药耐受性良好,最常见的不良反应为腹泻。8名可评估患者中有5名实现了前列腺特异性抗原(PSA)反应;2名患者的PSA检测不到且有影像学反应。一种新型的氯硝柳胺/PDMX1001重新配方与阿比特龙和泼尼松联合使用时达到了目标血浆水平,且耐受性良好。有必要对氯硝柳胺/PDMX1001的这种联合用药进行进一步研究。