Society for Nutrition, Education and Health Action, Mumbai, India.
UCL Institute for Global Health, London, UK.
Lancet Glob Health. 2017 Mar;5(3):e335-e349. doi: 10.1016/S2214-109X(16)30363-1.
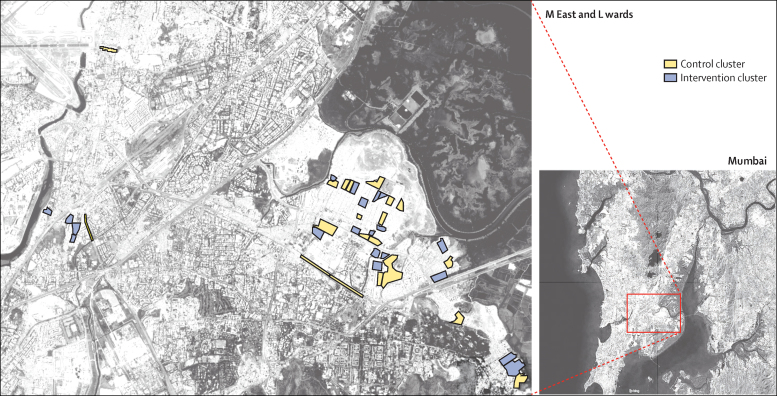
Around 105 million people in India will be living in informal settlements by 2017. We investigated the effects of local resource centres delivering integrated activities to improve women's and children's health in urban informal settlements.
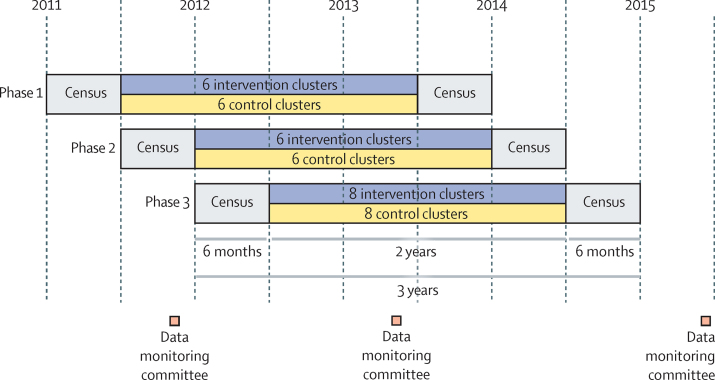
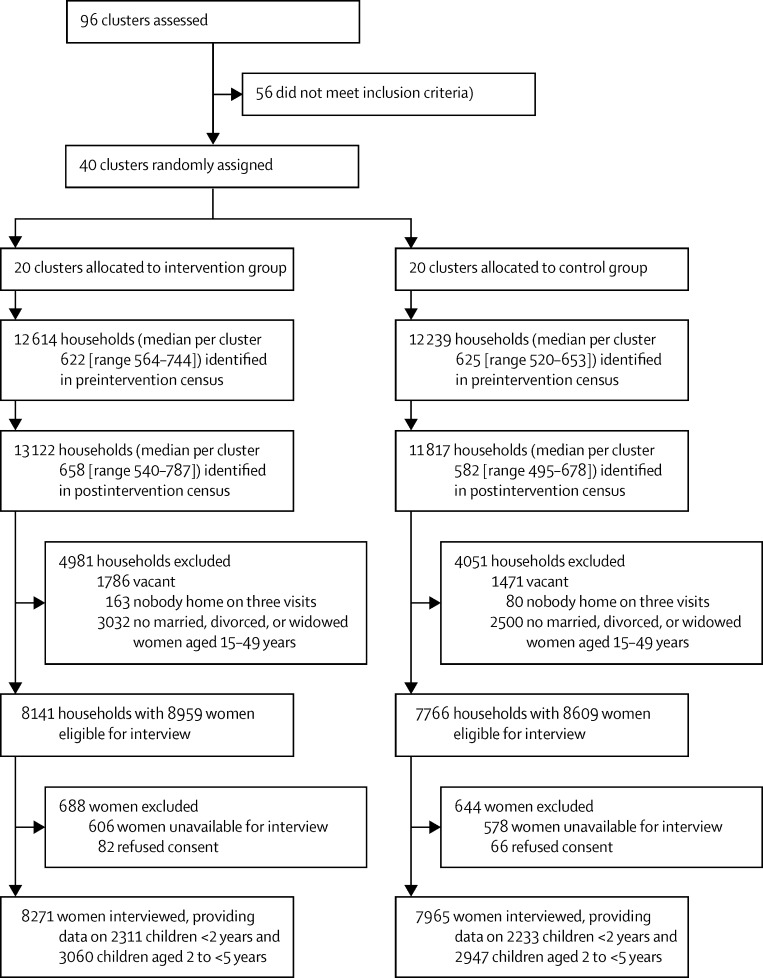
In a cluster-randomised controlled trial in 40 clusters, each containing around 600 households, 20 were randomly allocated to have a resource centre (intervention group) and 20 no centre (control group). Community organisers in the intervention centres addressed maternal and neonatal health, child health and nutrition, reproductive health, and prevention of violence against women and children through home visits, group meetings, day care, community events, service provision, and liaison. The primary endpoints were met need for family planning in women aged 15-49 years, proportion of children aged 12-23 months fully immunised, and proportion of children younger than 5 years with anthropometric wasting. Census interviews with women aged 15-49 years were done before and 2 years after the intervention was implemented. The primary intention-to-treat analysis compared cluster allocation groups after the intervention. We also analysed the per-protocol population (all women with data from both censuses) and assessed cluster-level changes. This study is registered with ISRCTN, number ISRCTN56183183, and Clinical Trials Registry of India, number CTRI/2012/09/003004.
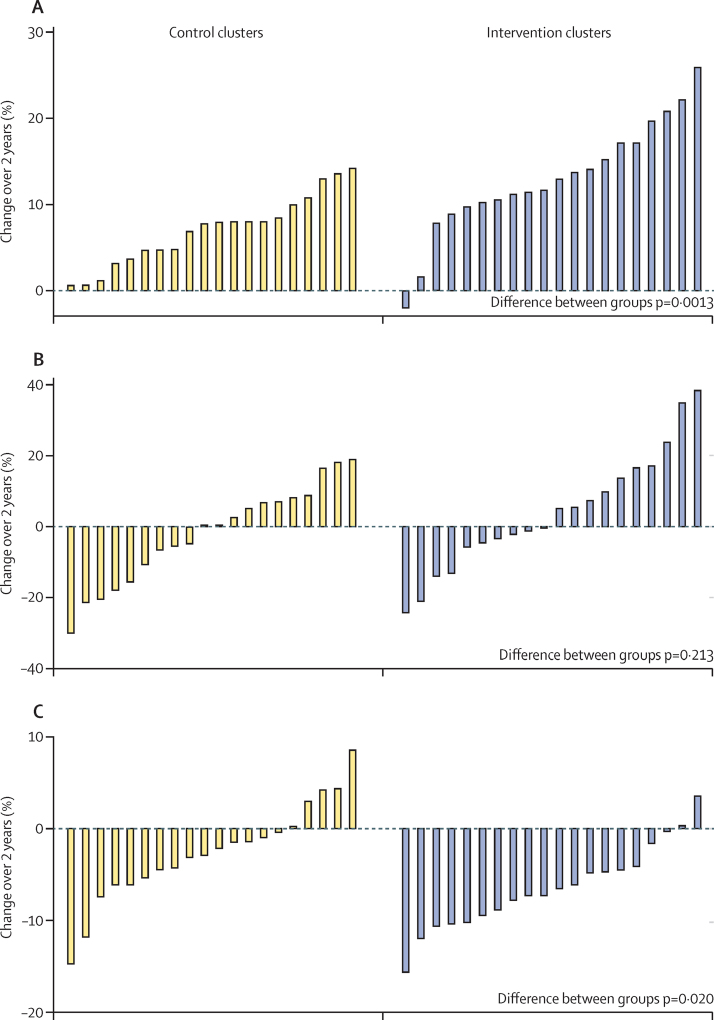
12 614 households were allocated to the intervention and 12 239 to control. Postintervention data were available for 8271 women and 5371 children younger than 5 years in the intervention group, and 7965 women and 5180 children in the control group. Met need for family planning was greater in the intervention clusters than in the control clusters (odds ratio [OR] 1·31, 95% CI 1·11-1·53). The proportions of fully immunised children were similar in the intervention and control groups in the intention-to-treat analysis (OR 1·30, 95% CI 0·84-2·01), but were greater in the intervention group when assessed per protocol (1·73, 1·05-2·86). Childhood wasting did not differ between groups (OR 0·92, 95% CI 0·75-1·12), although improvement was seen at the cluster level in the intervention group (p=0·020).
This community resource model seems feasible and replicable and may be protocolised for expansion.
Wellcome Trust, CRY, Cipla.
到 2017 年,印度将有大约 1.05 亿人居住在非正规住区。我们研究了地方资源中心提供综合活动,以改善城市非正规住区妇女和儿童健康的效果。
在一项 40 个集群的集群随机对照试验中,每个集群包含约 600 户家庭,其中 20 个集群被随机分配到有资源中心(干预组),20 个集群没有中心(对照组)。干预中心的社区组织者通过家访、小组会议、日托、社区活动、服务提供和联络,解决产妇和新生儿健康、儿童健康和营养、生殖健康以及预防暴力侵害妇女和儿童问题。主要终点是 15-49 岁妇女的计划生育需求、12-23 个月大的儿童完全免疫的比例以及 5 岁以下儿童消瘦的比例。在干预实施前和实施后 2 年对 15-49 岁的妇女进行了人口普查访谈。主要的意向治疗分析比较了干预后的集群分配组。我们还分析了方案人群(所有有两次人口普查数据的妇女)和评估了集群水平的变化。本研究在 ISRCTN 注册,编号 ISRCTN56183183,在印度临床试验注册处注册,编号 CTRI/2012/09/003004。
共有 12614 户家庭被分配到干预组,12239 户家庭被分配到对照组。干预组有 8271 名妇女和 5371 名 5 岁以下儿童,对照组有 7965 名妇女和 5180 名 5 岁以下儿童,在干预后获得了数据。与对照组相比,干预组的计划生育需求更高(比值比 [OR] 1.31,95%CI 1.11-1.53)。意向治疗分析中,完全免疫儿童的比例在干预组和对照组相似(OR 1.30,95%CI 0.84-2.01),但按方案评估时,干预组更高(1.73,1.05-2.86)。两组儿童消瘦的比例无差异(OR 0.92,95%CI 0.75-1.12),尽管干预组在集群层面有所改善(p=0.020)。
这种社区资源模式似乎可行且可复制,可以制定方案进行推广。
惠康信托基金会、CRY、西普拉。