Bress Adam P, Kramer Holly, Khatib Rasha, Beddhu Srinivasan, Cheung Alfred K, Hess Rachel, Bansal Vinod K, Cao Guichan, Yee Jerry, Moran Andrew E, Durazo-Arvizu Ramon, Muntner Paul, Cooper Richard S
From Division of Health System Innovation and Research, Department of Population Health Sciences, University of Utah School of Medicine, Salt Lake City (A.P.B., R.H.); Department of Public Health Sciences (H.K., R.K., G.C., R.D.-A., R.S.C.) and Division of Nephrology and Hypertension (H.K., V.K.B.), Loyola Medical Center, Maywood, IL; Division of Nephrology and Hypertension, University of Utah, Salt Lake City (S.B., A.K.C.); Division of General Internal Medicine, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City (R.H.); Division of Nephrology and Hypertension, Henry Ford Hospital, Detroit, MI (J.Y.); Division of General Medicine, Department of Medicine, Columbia University Medical Center, New York, NY (A.E.M.); and School of Public Health, Department of Epidemiology, University of Alabama at Birmingham (P.M.).
Circulation. 2017 Apr 25;135(17):1617-1628. doi: 10.1161/CIRCULATIONAHA.116.025322. Epub 2017 Feb 13.
SPRINT (Systolic Blood Pressure Intervention Trial) demonstrated a 27% reduction in all-cause mortality with a systolic blood pressure (SBP) goal of <120 versus <140 mm Hg among US adults at high cardiovascular disease risk but without diabetes mellitus, stroke, or heart failure. To quantify the potential benefits and risks of SPRINT intensive goal implementation, we estimated the deaths prevented and excess serious adverse events incurred if the SPRINT intensive SBP treatment goal were implemented in all eligible US adults.
SPRINT eligibility criteria were applied to the 1999 to 2006 National Health and Nutrition Examination Survey and linked with the National Death Index through December 2011. SPRINT eligibility included age ≥50 years, SBP of 130 to 180 mm Hg (depending on the number of antihypertensive medications being taken), and high cardiovascular disease risk. Exclusion criteria were diabetes mellitus, history of stroke, >1 g proteinuria, heart failure, estimated glomerular filtration rate <20 mL·min·1.73 m, or dialysis. Annual mortality rates were calculated by dividing the Kaplan-Meier 5-year mortality by 5. Hazard ratios for all-cause mortality and heart failure and absolute risks for serious adverse events in SPRINT were used to estimate the number of potential deaths and heart failure cases prevented and serious adverse events incurred with intensive SBP treatment.
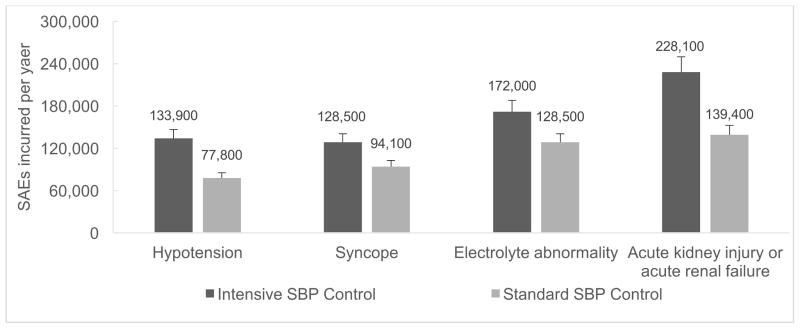
The mean age was 68.6 years, and 83.2% and 7.4% were non-Hispanic white and non-Hispanic black, respectively. The annual mortality rate was 2.20% (95% confidence interval [CI], 1.91-2.48), and intensive SBP treatment was projected to prevent ≈107 500 deaths per year (95% CI, 93 300-121 200) and give rise to 56 100 (95% CI, 50 800-61 400) episodes of hypotension, 34 400 (95% CI, 31 200-37 600) episodes of syncope, 43 400 (95% CI, 39 400-47 500) serious electrolyte disorders, and 88 700 (95% CI, 80 400-97 000) cases of acute kidney injury per year. The analysis-of-extremes approach indicated that the range of estimated lower- and upper-bound number of deaths prevented per year with intensive SBP control was 34 600 to 179 600. Intensive SBP control was projected to prevent 46 100 (95% CI, 41 800-50 400) cases of heart failure annually.
If fully implemented in eligible US adults, intensive SBP treatment could prevent ≈107 500 deaths per year. A consequence of this treatment strategy, however, could be an increase in serious adverse events.
收缩压干预试验(SPRINT)表明,在美国心血管疾病高风险但无糖尿病、中风或心力衰竭的成年人中,将收缩压(SBP)目标设定为<120 mmHg对比<140 mmHg可使全因死亡率降低27%。为了量化实施SPRINT强化目标的潜在益处和风险,我们估计了如果在美国所有符合条件的成年人中实施SPRINT强化SBP治疗目标可预防的死亡人数以及由此产生的额外严重不良事件。
将SPRINT纳入标准应用于1999年至2006年的美国国家健康与营养检查调查,并与截至2011年12月的国家死亡指数相联系。SPRINT纳入标准包括年龄≥50岁、SBP为130至180 mmHg(取决于正在服用的抗高血压药物数量)以及心血管疾病高风险。排除标准为糖尿病、中风病史、蛋白尿>1 g、心力衰竭、估计肾小球滤过率<20 mL·min·1.73 m或透析。通过将Kaplan-Meier 5年死亡率除以5来计算年死亡率。使用SPRINT中全因死亡率和心力衰竭的风险比以及严重不良事件的绝对风险来估计强化SBP治疗可预防的潜在死亡人数和心力衰竭病例数以及由此产生的严重不良事件。
平均年龄为68.6岁,分别有83.2%和7.4%为非西班牙裔白人和非西班牙裔黑人。年死亡率为2.20%(95%置信区间[CI],1.91 - 2.48),强化SBP治疗预计每年可预防约107500例死亡(95% CI,93300 - 121200),并导致每年发生56100例(95% CI,50800 - 61400)低血压、34400例(95% CI,31200 - 37600)晕厥、43400例(95% CI,39400 - 47500)严重电解质紊乱以及88700例(95% CI,80400 - 97000)急性肾损伤。极端值分析方法表明,强化SBP控制每年预防死亡人数的估计下限和上限范围为34600至179600例。强化SBP控制预计每年可预防46100例(95% CI,41800 - 50400)心力衰竭病例。
如果在美国符合条件的成年人中全面实施,强化SBP治疗每年可预防约107500例死亡。然而,这种治疗策略的一个后果可能是严重不良事件的增加。