Di Pollina Laura, Guessous Idris, Petoud Véronique, Combescure Christophe, Buchs Bertrand, Schaller Philippe, Kossovsky Michel, Gaspoz Jean-Michel
Division of Primary Care Medicine, Department of Community Medicine, Primary Care and Emergency Medicine, Geneva University Hospitals, 1, avenue Calas, Geneva, 1206, Switzerland.
Department of Ambulatory Care and Community Medicine, University of Lausanne, Lausanne, Switzerland.
BMC Geriatr. 2017 Feb 14;17(1):53. doi: 10.1186/s12877-017-0449-9.
Care of frail and dependent older adults with multiple chronic conditions is a major challenge for health care systems. The study objective was to test the efficacy of providing integrated care at home to reduce unnecessary hospitalizations, emergency room visits, institutionalization, and mortality in community dwelling frail and dependent older adults.
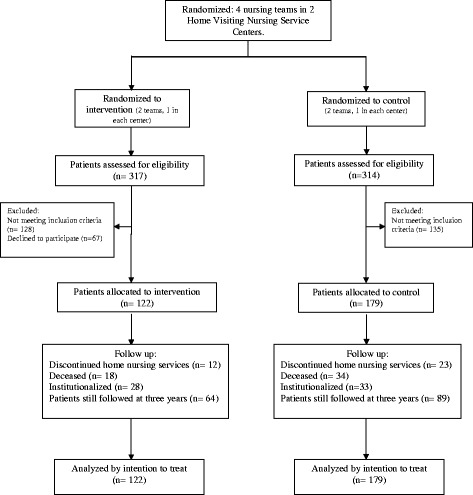
A prospective controlled trial was conducted, in real-life clinical practice settings, in a suburban region in Geneva, Switzerland, served by two home visiting nursing service centers. Three hundred and one community-dwelling frail and dependent people over 60 years old were allocated to previously randomized nursing teams into Control (N = 179) and Intervention (N = 122) groups: Controls received usual care by their primary care physician and home visiting nursing services, the Intervention group received an additional home evaluation by a community geriatrics unit with access to a call service and coordinated follow-up. Recruitment began in July 2009, goals were obtained in July 2012, and outcomes assessed until December 2012. Length of follow-up ranged from 5 to 41 months (mean 16.3). Primary outcome measure was the number of hospitalizations. Secondary outcomes were reasons for hospitalizations, the number and reason of emergency room visits, institutionalization, death, and place of death.
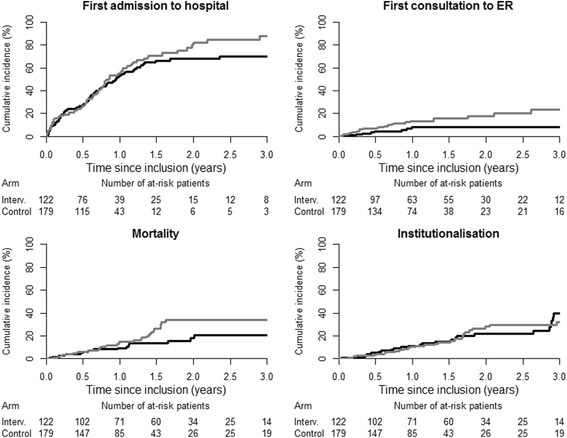
The number of hospitalizations did not differ between groups however, the intervention led to lower cumulative incidence for the first hospitalization after the first year of follow-up (69.8%, CI 59.9 to 79.6 versus 87 · 6%, CI 78 · 2 to 97 · 0; p = .01). Secondary outcomes showed that the intervention compared to the control group had less frequent unnecessary hospitalizations (4.1% versus 11.7%, p = .03), lower cumulative incidence for the first emergency room visit, 8.3%, CI 2.6 to 13.9 versus 23.2%, CI 13.1 to 33.3; p = .01), and death occurred more frequently at home (44.4 versus 14.7%; p = .04). No significant differences were found for institutionalization and mortality.
Integrated care that included a home visiting multidisciplinary geriatric team significantly reduced unnecessary hospitalizations, emergency room visits and allowed more patients to die at home. It is an effective tool to improve coordination and access to care for frail and dependent older adults.
Clinical Trials.gov Identifier: NCT02084108 . Retrospectively registered on March 10 2014.
照顾患有多种慢性病的体弱且依赖他人的老年人是医疗保健系统面临的一项重大挑战。本研究的目的是测试在家中提供综合护理以减少社区居住的体弱且依赖他人的老年人不必要的住院、急诊就诊、机构化安置和死亡的效果。
在瑞士日内瓦的一个郊区的实际临床实践环境中,由两个上门护理服务中心开展了一项前瞻性对照试验。301名60岁以上社区居住的体弱且依赖他人的人被分配到之前随机分组的护理团队,分为对照组(N = 179)和干预组(N = 122):对照组接受初级保健医生的常规护理和上门护理服务,干预组由社区老年病科进行额外的家庭评估,并可使用呼叫服务和进行协调随访。招募工作于2009年7月开始,2012年7月达成目标,并持续评估结果至2012年12月。随访时间从5个月到41个月不等(平均16.3个月)。主要结局指标是住院次数。次要结局包括住院原因、急诊就诊次数和原因、机构化安置、死亡以及死亡地点。
两组之间的住院次数没有差异,然而,干预导致随访第一年之后首次住院的累积发生率较低(69.8%,CI 59.9至79.6与87.6%,CI 78.2至97.0;p = 0.01)。次要结局显示,与对照组相比,干预组不必要住院的频率更低(4.1%对11.7%,p = 0.03),首次急诊就诊的累积发生率更低,8.·3%,CI 2.6至13.9与23.2%,CI 13.1至33.3;p = 0.01),且在家中死亡的情况更常见(44.4%对14.7%;p = 0.04)。在机构化安置和死亡率方面未发现显著差异。
包括上门多学科老年护理团队的综合护理显著减少了不必要的住院、急诊就诊,并使更多患者在家中死亡。这是改善体弱且依赖他人的老年人护理协调和可及性的有效工具。
ClinicalTrials.gov标识符:NCT02084108。于2014年3月10日进行回顾性注册。