Laquente Berta, Lopez-Martin Jose, Richards Donald, Illerhaus Gerald, Chang David Z, Kim George, Stella Philip, Richel Dirk, Szcylik Cezary, Cascinu Stefano, Frassineti G L, Ciuleanu Tudor, Hurt Karla, Hynes Scott, Lin Ji, Lin Aimee Bence, Von Hoff Daniel, Calvo Emiliano
Institut Català d'Oncologia-IDIBELL (Institut d'Investigació Biomèdica de Bellvitge), Barcelona, Spain.
University Hospital and Research Institute, Madrid, Spain.
BMC Cancer. 2017 Feb 15;17(1):137. doi: 10.1186/s12885-017-3131-x.
The aim of this study was to determine whether checkpoint kinase 1 inihibitor (CHK1), LY2603618, and gemcitabine prolong overall survival (OS) compared to gemcitabine alone in patients with unresectable pancreatic cancer.
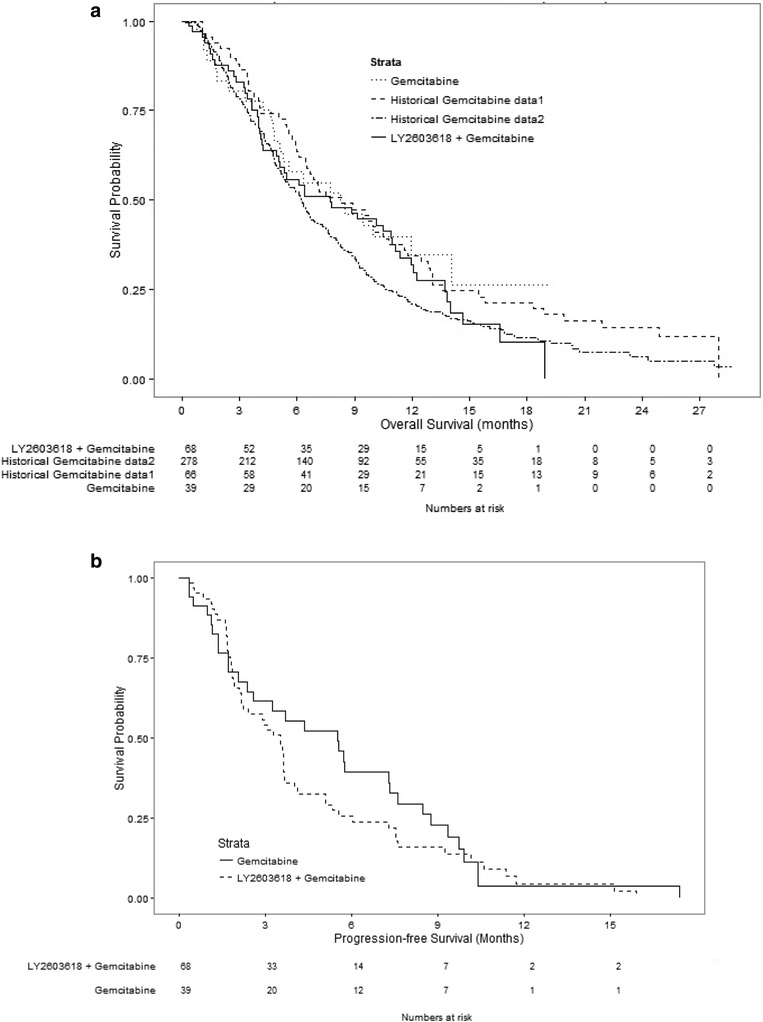
Patients with Stage II-IV locally advanced or metastatic pancreatic cancer were randomized (2:1) to either 230 mg of LY2603618/1000 mg/m gemcitabine combined or 1000 mg/m gemcitabine alone. OS was assessed using both a Bayesian augment control model and traditional frequentist analysis for inference. Progression-free survival (PFS), overall response rate (ORR), duration of response, pharmacokinetics (PK), and safety (Common Terminology Criteria for Adverse Events [AEs] v 3.0) were also evaluated.
Ninety-nine patients (n = 65, LY2603618/gemcitabine; n = 34, gemcitabine) were randomized (intent-to-treat population). The median OS (months) was 7.8 (range, 0.3-18.9) with LY2603618/gemcitabine and 8.3 (range, 0.8-19.1+) with gemcitabine. Similarly, in a Bayesian analysis, the study was not positive since the posterior probability that LY2603618/gemcitabine was superior to gemcitabine in improving OS was 0.3, which did not exceed the prespecified threshold of 0.8. No significant improvements in PFS, ORR, or duration of response were observed. Drug-related treatment-emergent AEs in both arms included nausea, thrombocytopenia, fatigue, and neutropenia. The severity of AEs with LY2603618/gemcitabine was comparable to gemcitabine. The LY2603618 exposure targets (AUC ≥21,000 ng∙hr/mL and C ≥2000 ng/mL) predicted for maximum pharmacodynamic response were achieved after 230 mg of LY2603618.
LY2603618/gemcitabine was not superior to gemcitabine for the treatment of patients with pancreatic cancer.
NCT00839332 . Clinicaltrials.gov. Date of registration: 6 February 2009.
本研究旨在确定与单独使用吉西他滨相比,检查点激酶1抑制剂(CHK1)LY2603618与吉西他滨联合使用是否能延长不可切除胰腺癌患者的总生存期(OS)。
将II-IV期局部晚期或转移性胰腺癌患者按2:1随机分组,分别接受230mg的LY2603618/1000mg/m²吉西他滨联合治疗或单独使用1000mg/m²吉西他滨。使用贝叶斯增强对照模型和传统频率分析进行推断,评估总生存期(OS)。还评估了无进展生存期(PFS)、总缓解率(ORR)、缓解持续时间、药代动力学(PK)和安全性(不良事件通用术语标准[AEs] v3.0)。
99例患者(n = 65,LY2603618/吉西他滨组;n = 34,吉西他滨组)被随机分组(意向性治疗人群)。LY2603618/吉西他滨组的中位总生存期(月)为7.8(范围0.3-18.9),吉西他滨组为8.3(范围0.8-19.1+)。同样,在贝叶斯分析中,该研究结果为阴性,因为LY2603618/吉西他滨在改善总生存期方面优于吉西他滨的后验概率为0.3,未超过预先设定的0.8阈值。未观察到无进展生存期、总缓解率或缓解持续时间有显著改善。两组与药物相关的治疗中出现的不良事件包括恶心、血小板减少、疲劳和中性粒细胞减少。LY2603618/吉西他滨组不良事件的严重程度与吉西他滨组相当。在给予230mg的LY2603618后,达到了预测最大药效学反应的LY2603618暴露目标(AUC≥21,000ng∙hr/mL和C≥2000ng/mL)。
LY2603618/吉西他滨在治疗胰腺癌患者方面并不优于吉西他滨。
NCT00839332。Clinicaltrials.gov。注册日期:2009年2月6日。