Oksman Erja, Linna Miika, Hörhammer Iiris, Lammintakanen Johanna, Talja Martti
Päijät-Häme Social and Health Care District, Keskussairaalankatu 7, 15 850, Lahti, Finland.
Healthcare Engineering, Management and Architecture Institute, Aalto University, Espoo, Finland.
BMC Health Serv Res. 2017 Feb 15;17(1):138. doi: 10.1186/s12913-017-2088-4.
The burden of chronic disease and multimorbidity is rapidly increasing. Self-management support interventions are effective in reduce cost, especially when targeted at a single disease group; however, economical evidence of such complex interventions remains scarce. The objective of this study was to evaluate a cost-effectiveness analysis of a tele-based health-coaching intervention among patients with type 2 diabetes (T2D), coronary artery disease (CAD) and congestive heart failure (CHF).
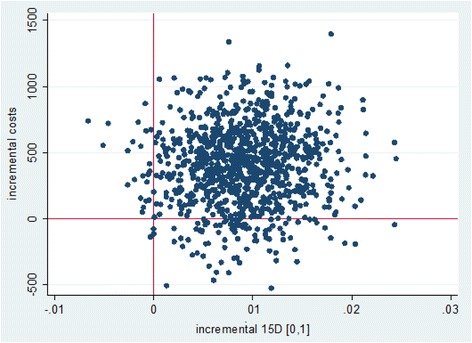
A total of 1570 patients were blindly randomized to intervention (n = 970) and control (n = 470) groups. The intervention group received monthly individual health coaching by telephone from a specially trained nurse for 12-months in addition to routine social and healthcare. Patients in the control group received routine social and health care. Quality of life was assessed at the beginning of the intervention and follow-up measurements were made after 12 months health coaching. The cost included all direct health-care costs supplemented with home care and nursing home-care costs in social care. Utility was based on a Health Related Quality of Life (HRQoL) measurement (15D instrument), and cost effectiveness was assessed using incremental cost-effectiveness ratios (ICERs).
The cost-effectiveness of health coaching was highest in the T2D group (ICER €20,000 per Quality-Adjusted Life Years [QALY]). The ICER for the CAD group was more modest (€40,278 per QALY), and in the CHF group, costs increased with no marked effect on QoL. Probabilistic sensitivity analysis indicated that at the societal willingness to pay threshold of €50,000 per QALY, the probability of health coaching being cost effective was 55% in the whole study group.
The cost effectiveness of health coaching may vary substantially across patient groups, and thus interventions should be targeted at selected subgroups of chronically ill. Based on the results of this study, health coaching improved the QoL of T2D and CAD patients with moderate costs. However, the results are grounded on a short follow-up period, and more evidence is needed to evaluate the long-term outcomes of health-coaching programs.
NCT00552903 [Prospectively registered, registration date 1 November 2007, last updated 3 February 2009].
慢性病和多种疾病并存的负担正在迅速增加。自我管理支持干预措施在降低成本方面是有效的,特别是针对单一疾病群体时;然而,此类复杂干预措施的经济学证据仍然稀缺。本研究的目的是评估一项基于远程健康指导干预对2型糖尿病(T2D)、冠状动脉疾病(CAD)和充血性心力衰竭(CHF)患者的成本效益分析。
总共1570名患者被随机分为干预组(n = 970)和对照组(n = 470)。干预组除接受常规社会和医疗保健外,还由经过专门培训的护士每月通过电话进行为期12个月的个人健康指导。对照组患者接受常规社会和医疗保健。在干预开始时评估生活质量,并在12个月的健康指导后进行随访测量。成本包括所有直接医疗保健成本,并补充了社会护理中的家庭护理和养老院护理成本。效用基于健康相关生活质量(HRQoL)测量(15D工具),并使用增量成本效益比(ICER)评估成本效益。
健康指导的成本效益在T2D组中最高(每质量调整生命年[QALY]的ICER为20,000欧元)。CAD组的ICER较为适度(每QALY为40,278欧元),而在CHF组中,成本增加但对生活质量没有明显影响。概率敏感性分析表明,在社会每QALY支付意愿阈值为50,000欧元时,健康指导具有成本效益的概率在整个研究组中为55%。
健康指导的成本效益在不同患者群体中可能有很大差异,因此干预措施应针对特定的慢性病亚组。基于本研究结果,健康指导以适度成本改善了T2D和CAD患者的生活质量。然而,这些结果基于较短的随访期,需要更多证据来评估健康指导计划的长期结果。
NCT00552903 [前瞻性注册,注册日期2007年11月1日,最后更新日期2009年2月3日]