Goorts Briete, van Nijnatten Thiemo J A, de Munck Linda, Moossdorff Martine, Heuts Esther M, de Boer Maaike, Lobbes Marc B I, Smidt Marjolein L
GROW - School for Oncology and Developmental Biology, Maastricht University Medical Centre, Maastricht, The Netherlands.
Department of Surgery, Maastricht University Medical Centre, P.O. Box 5800, 6202 AZ, Maastricht, The Netherlands.
Breast Cancer Res Treat. 2017 May;163(1):83-91. doi: 10.1007/s10549-017-4155-2. Epub 2017 Feb 15.
Pathological complete response (pCR) is the ultimate response in breast cancer patients treated with neoadjuvant chemotherapy (NCT). It might be a surrogate outcome for disease-free survival (DFS) and overall survival (OS). We studied the effect of clinical tumor stage (cT-stage) on tumor pCR and the effect of pCR per cT-stage on 5-year OS and DFS.
Using the Netherlands Cancer Registry, all primary invasive breast cancer patients treated with NCT from 2005 until 2008 were identified. Univariable logistic regression analysis was performed to evaluate the effect of cT-stage on pCR, stepwise logistic regression analysis to correct for potential confounders and Kaplan-Meier survival analyses to calculate OS and DFS after five years.
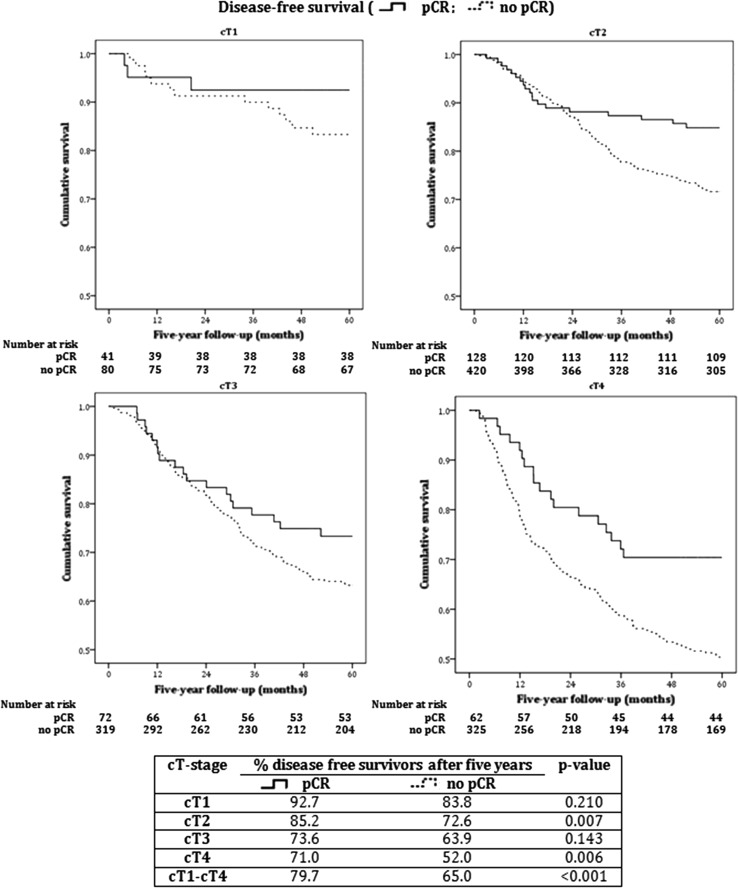
In 2366 patients, overall pCR rate was 21%. For cT1, cT2, cT3, and cT4, pCR rates were 31, 22, 18, and 17%, respectively. Lower cT-stage (cT1-2 vs cT3-4) was a significant independent predictor of higher pCR rate (p < 0.001, OR 3.15). Furthermore, positive HER2 status (p < 0.001, OR 2.30), negative estrogen receptor status (p = 0.062, OR 1.69), and negative progesterone receptor status (p = 0.008, OR 2.27) were independent predictors of pCR. OS and DFS were up to 20% higher in patients with cT2-4 tumors with pCR versus patients without pCR. DFS was also higher for cT1 tumors with pCR.
The most important predictor of pCR in breast cancer patients is cT-stage: lower cT-stages have significantly higher pCR rates than higher cT-stages. Patients with cT2-4 tumors achieving pCR have higher OS and DFS compared to patients not achieving pCR.
病理完全缓解(pCR)是接受新辅助化疗(NCT)的乳腺癌患者的最终反应。它可能是无病生存期(DFS)和总生存期(OS)的替代结局。我们研究了临床肿瘤分期(cT分期)对肿瘤pCR的影响以及每个cT分期的pCR对5年OS和DFS的影响。
利用荷兰癌症登记处,确定了2005年至2008年期间所有接受NCT治疗的原发性浸润性乳腺癌患者。进行单变量逻辑回归分析以评估cT分期对pCR的影响,进行逐步逻辑回归分析以校正潜在混杂因素,并进行Kaplan-Meier生存分析以计算5年后的OS和DFS。
在2366例患者中,总体pCR率为21%。对于cT1、cT2、cT3和cT4,pCR率分别为31%、22%、18%和17%。较低的cT分期(cT1-2与cT3-4相比)是较高pCR率的显著独立预测因素(p<0.001,OR 3.15)。此外,HER2阳性状态(p<0.001,OR 2.30)、雌激素受体阴性状态(p = 0.062,OR 1.69)和孕激素受体阴性状态(p = 0.008,OR 2.27)是pCR的独立预测因素。与无pCR的患者相比,cT2-4期肿瘤达到pCR的患者的OS和DFS高出20%。cT1期肿瘤达到pCR的患者的DFS也更高。
乳腺癌患者pCR的最重要预测因素是cT分期:较低的cT分期的pCR率明显高于较高的cT分期。与未达到pCR的患者相比,cT2-4期肿瘤达到pCR的患者具有更高的OS和DFS。