Fox Erin E, Holcomb John B, Wade Charles E, Bulger Eileen M, Tilley Barbara C
*Center for Translational Injury Research, Division of Acute Care Surgery, Department of Surgery, McGovern Medical School, University of Texas Health Science Center at Houston, Houston, Texas †Division of Trauma and Critical Care, Department of Surgery, School of Medicine, University of Washington, Seattle, Washington ‡Division of Biostatistics, School of Public Health, University of Texas Health Science Center at Houston, Houston, Texas.
Shock. 2017 May;47(5):567-573. doi: 10.1097/SHK.0000000000000788.
Choosing the appropriate endpoint for a trauma hemorrhage control trial can determine the likelihood of its success. Recent Phase 3 trials and observational studies have used 24-h and/or 30-day all-cause mortality as the primary endpoint and some have not used exception from informed consent (EFIC), resulting in multiple failed trials. Five recent high-quality prospective studies among 4,064 hemorrhaging trauma patients provide new evidence to support earlier primary endpoints.
The goal of this project was to determine the optimal endpoint for hemorrhage control trials using existing literature and new analyses of previously published data.
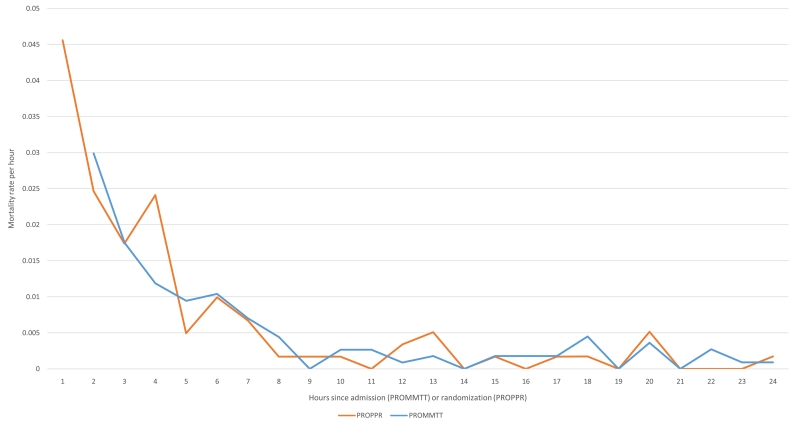
Recent studies among bleeding trauma patients show that hemorrhagic deaths occur rapidly, at a high rate, and in a consistent pattern. Early preventable deaths among trauma patients are largely due to hemorrhage and the median time to hemorrhagic death from admission is 2.0 to 2.6 h. Approximately 85% of hemorrhagic deaths occur within 6 h. The hourly mortality rate due to traumatic injury decreases rapidly after enrollment from 4.6% per hour at 1 hour postenrollment to 1% per hour at 6 h to <0.1% per hour by 9 h and thereafter. Early primary endpoints (within 6 h) have critically important benefits for hemorrhage control trials, including being congruent with the median time to hemorrhagic death, biologic plausibility, and enabling the use of all-cause mortality, which is definitive and objective.
Primary endpoints should be congruent with the timing of the disease process. Therefore, if a resuscitation/hemorrhage control intervention is under study, a primary endpoint of all-cause mortality evaluated within the first 6 h is appropriate. Before choosing the timing of the primary endpoint for a large multicenter trial, we recommend performing a Phase 2 trial under EFIC to better understand the effects of the hemorrhage control intervention and distribution of time to death. When early primary endpoints are used, patients should be monitored for multiple subsequent secondary safety endpoints, including 24 h and 30-day all-cause mortality as well as the customary safety endpoints.
为创伤出血控制试验选择合适的终点可决定其成功的可能性。近期的3期试验和观察性研究将24小时和/或30天全因死亡率作为主要终点,且一些研究未采用知情同意豁免(EFIC),导致多项试验失败。近期在4064例出血性创伤患者中开展的五项高质量前瞻性研究提供了支持更早主要终点的新证据。
本项目的目标是利用现有文献和对既往发表数据的新分析来确定出血控制试验的最佳终点。
近期对出血性创伤患者的研究表明,出血性死亡发生迅速、发生率高且模式一致。创伤患者早期可预防的死亡主要归因于出血,入院至出血性死亡的中位时间为2.0至2.6小时。约85%的出血性死亡发生在6小时内。创伤性损伤导致的每小时死亡率在入组后迅速下降,从入组后1小时的每小时4.6%降至6小时的每小时1%,至9小时及以后降至每小时<0.1%。早期主要终点(6小时内)对出血控制试验具有至关重要的益处,包括与出血性死亡的中位时间一致、生物学合理性,以及能够使用确定性和客观性的全因死亡率。
主要终点应与疾病进程的时间一致。因此,如果正在研究复苏/出血控制干预措施,在前6小时内评估全因死亡率作为主要终点是合适的。在为大型多中心试验选择主要终点的时间之前,我们建议在EFIC下开展2期试验,以更好地了解出血控制干预措施的效果和死亡时间分布。当使用早期主要终点时,应监测患者多个后续的次要安全性终点,包括24小时和30天全因死亡率以及常规的安全性终点。