Stankov Ivana, Howard Natasha J, Daniel Mark, Cargo Margaret
Urban Health Collaborative, Dornsife School of Public Health, Drexel University, Philadelphia, PA 19104, USA.
Centre for Population Health Research, School of Health Sciences, University of South Australia, Adelaide, SA 5001, Australia.
Int J Environ Res Public Health. 2017 Feb 9;14(2):170. doi: 10.3390/ijerph14020170.
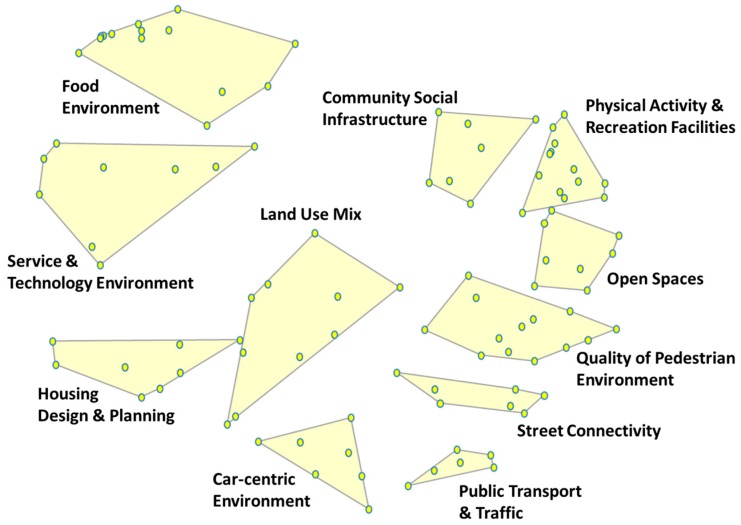
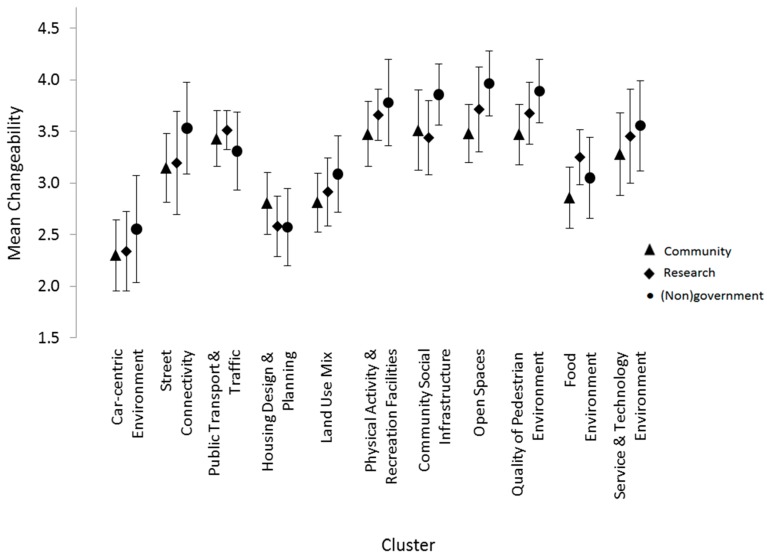
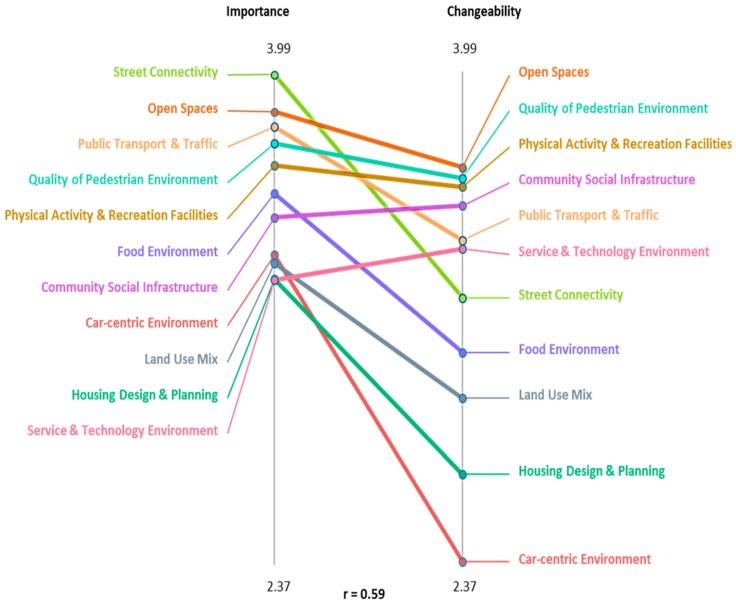
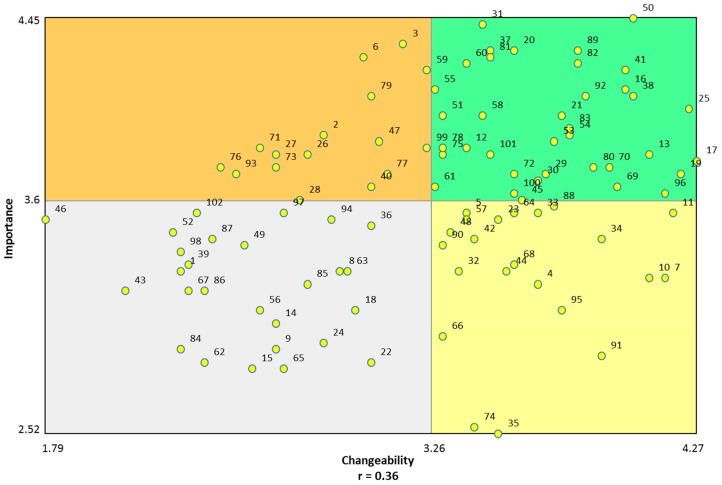
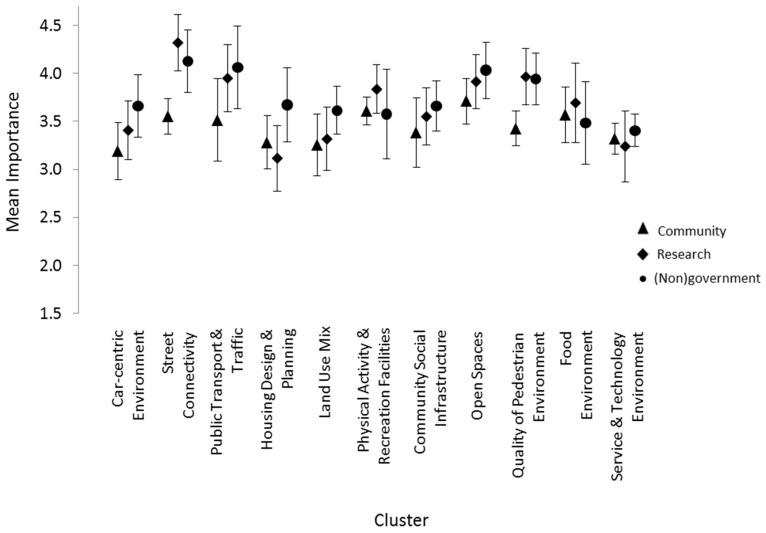
An underrepresentation of stakeholder perspectives within urban health research arguably limits our understanding of what is a multi-dimensional and complex relationship between the built environment and health. By engaging a wide range of stakeholders using a participatory concept mapping approach, this study aimed to achieve a more holistic and nuanced understanding of the built environments shaping disease risk, specifically cardiometabolic risk (CMR). Moreover, this study aimed to ascertain the importance and changeability of identified environments through government action. Through the concept mapping process, community members, researchers, government and non-government stakeholders collectively identified eleven clusters encompassing 102 built environmental domains related to CMR, a number of which are underrepresented within the literature. Among the identified built environments, open space, public transportation and pedestrian environments were highlighted as key targets for policy intervention. Whilst there was substantive convergence in stakeholder groups' perspectives concerning the built environment and CMR, there were disparities in the level of importance government stakeholders and community members respectively assigned to pedestrian environments and street connectivity. These findings support the role of participatory methods in strengthening how urban health issues are understood and in affording novel insights into points of action for public health and policy intervention.
城市健康研究中利益相关者观点的代表性不足,可以说限制了我们对建筑环境与健康之间多维复杂关系的理解。通过采用参与式概念图方法让广泛的利益相关者参与进来,本研究旨在更全面、细致地理解塑造疾病风险,特别是心血管代谢风险(CMR)的建筑环境。此外,本研究旨在通过政府行动确定已识别环境的重要性和可变性。通过概念图绘制过程,社区成员、研究人员、政府和非政府利益相关者共同确定了11个集群,涵盖与CMR相关的102个建筑环境领域,其中一些在文献中的代表性不足。在已识别的建筑环境中,开放空间、公共交通和行人环境被突出作为政策干预的关键目标。虽然利益相关者群体对建筑环境和CMR的观点存在实质性趋同,但政府利益相关者和社区成员分别赋予行人环境和街道连通性的重要性水平存在差异。这些发现支持了参与式方法在加强对城市健康问题的理解以及为公共卫生和政策干预的行动点提供新见解方面的作用。