Saw Swee Hock School of Public Health, National University Health System, National University of Singapore, Singapore.
Biodefence Centre, Singapore Armed Forces, Singapore.
Sci Rep. 2017 Feb 20;7:42963. doi: 10.1038/srep42963.
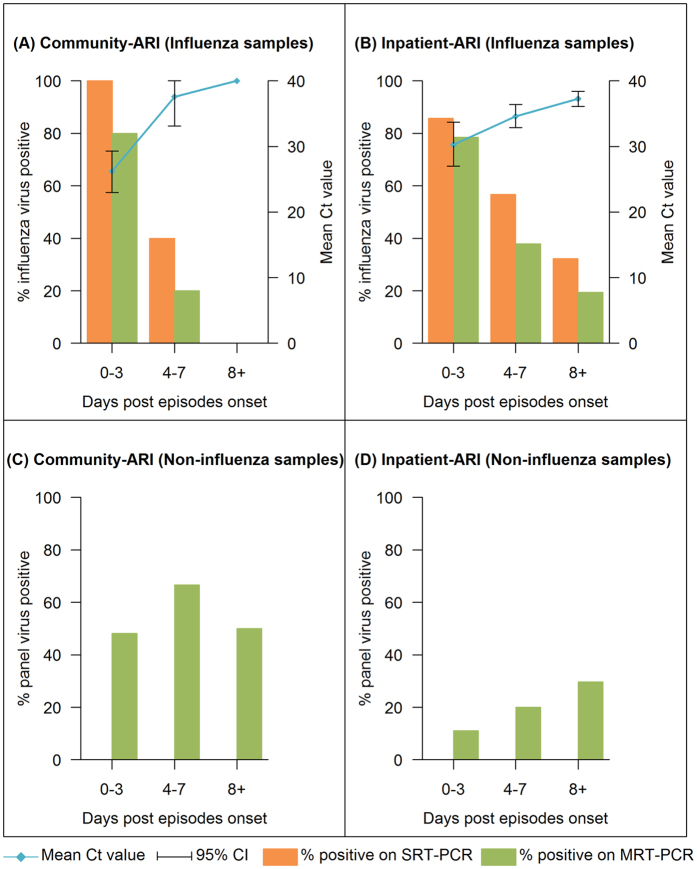
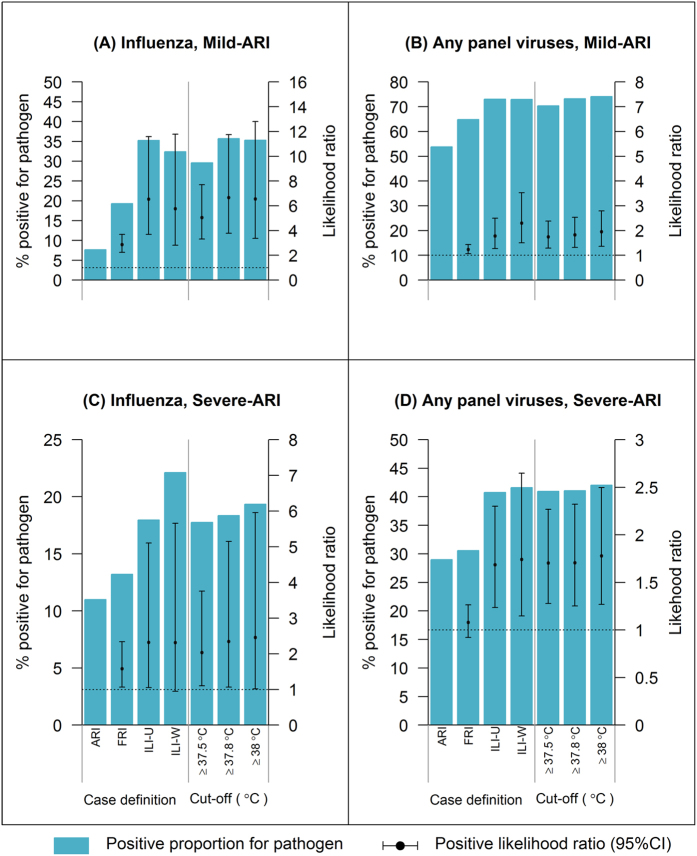
To investigate the performance of laboratory methods and clinical case definitions in detecting the viral pathogens for acute respiratory infections (ARIs) from a prospective community cohort and hospital inpatients, nasopharyngeal swabs from cohort members reporting ARIs (community-ARI) and inpatients admitted with ARIs (inpatient-ARI) were tested by Singleplex Real Time-Polymerase Chain Reaction (SRT-PCR), multiplex RT-PCR (MRT-PCR) and pathogen-chip system (PathChip) between April 2012 and December 2013. Community-ARI and inpatient-ARI was also combined with mild and severe cases of influenza from a historical prospective study as mild-ARI and severe-ARI respectively to evaluate the performance of clinical case definitions. We analysed 130 community-ARI and 140 inpatient-ARI episodes (5 inpatient-ARI excluded because multiple pathogens were detected), involving 138 and 207 samples respectively. Detection by PCR declined with days post-onset for influenza virus; decrease was faster for community-ARI than for inpatient-ARI. No such patterns were observed for non-influenza respiratory virus infections. PathChip added substantially to viruses detected for community-ARI only. Clinical case definitions discriminated influenza from other mild-ARI but performed poorly for severe-ARI and for older participants. Rational strategies for diagnosis and surveillance of influenza and other respiratory virus must acknowledge the differences between ARIs presenting in community and hospital settings.
为了研究实验室方法和临床病例定义在检测急性呼吸道感染(ARI)的病毒病原体方面的表现,我们对 2012 年 4 月至 2013 年 12 月期间报告 ARI(社区 ARI)的队列成员和因 ARI 住院的住院患者(住院 ARI)的鼻咽拭子进行了单重实时聚合酶链反应(SRT-PCR)、多重 RT-PCR(MRT-PCR)和病原体芯片系统(PathChip)检测。社区 ARI 和住院 ARI 还与历史前瞻性研究中轻度和重度流感病例合并,分别作为轻度 ARI 和重度 ARI 来评估临床病例定义的性能。我们分析了 130 例社区 ARI 和 140 例住院 ARI 发作(5 例住院 ARI 因检测到多种病原体而被排除),分别涉及 138 例和 207 例样本。流感病毒的 PCR 检测随发病后天数而下降;社区 ARI 的下降速度快于住院 ARI。对于非流感呼吸道病毒感染,未观察到这种模式。PathChip 仅为社区 ARI 增加了大量检测到的病毒。临床病例定义可区分流感与其他轻度 ARI,但对重度 ARI 和老年参与者的区分效果不佳。对于流感和其他呼吸道病毒的诊断和监测,合理的策略必须认识到社区和医院环境中出现的 ARI 之间的差异。