Pili Roberto, Liu Glenn, Chintala Sreenivasulu, Verheul Hendrick, Rehman Shabnam, Attwood Kristopher, Lodge Martin A, Wahl Richard, Martin James I, Miles Kiersten Marie, Paesante Silvia, Adelaiye Remi, Godoy Alejandro, King Serina, Zwiebel James, Carducci Michael A
Genitourinary Program, Indiana University-Simon Cancer Center, Indianapolis, IN, USA.
University of Wisconsin Carbone Cancer Center, Wisconsin, WI, USA.
Br J Cancer. 2017 Mar 28;116(7):874-883. doi: 10.1038/bjc.2017.33. Epub 2017 Feb 21.
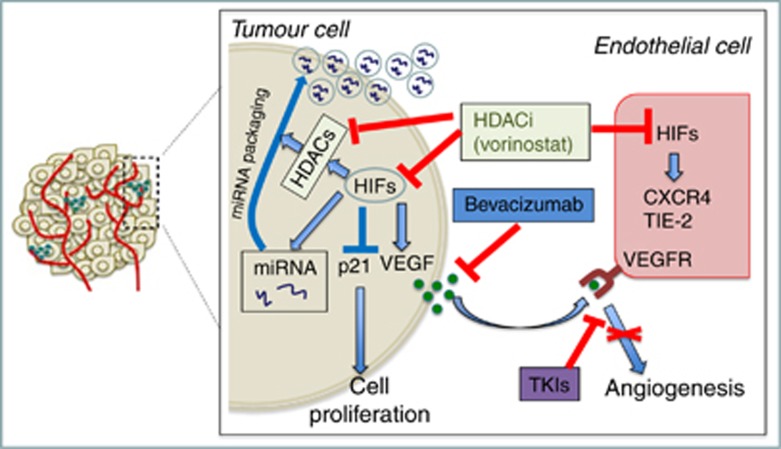
Class II histone deacetylase (HDAC) inhibitors induce hypoxia-inducible factor-1 and -2α degradation and have antitumour effects in combination with vascular endothelial growth factor (VEGF) inhibitors. In this study, we tested the safety and efficacy of the HDAC inhibitor vorinostat and the VEGF blocker bevacizumab in metastatic clear-cell renal cell carcinoma (ccRCC) patients previously treated with different drugs including sunitinib, sorafenib, axitinib, interleukin-2, interferon, and temsirolimus.
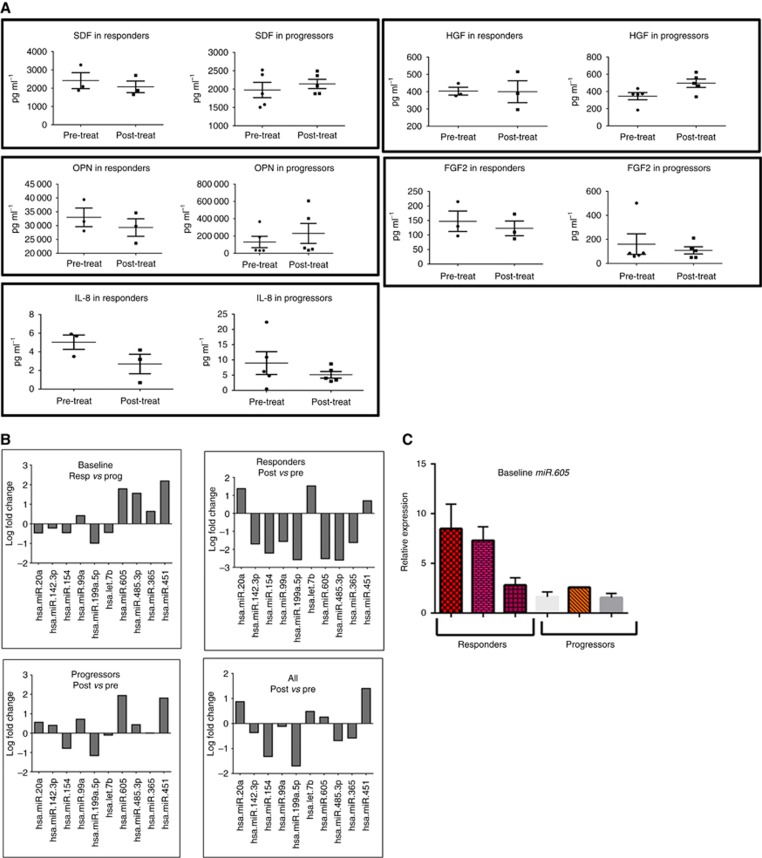
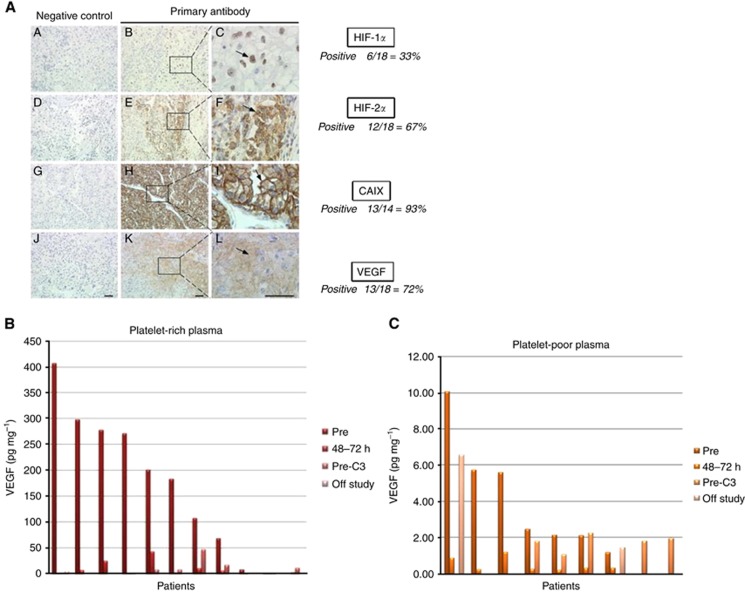
Patients with up to two prior regimens were eligible for treatment, consisting of vorinostat 200 mg orally two times daily × 2 weeks, and bevacizumab 15 mg kg intravenously every 3 weeks. The primary end points were safety and tolerability, and the proportion of patients with 6 months of progression-free survival (PFS). Correlative studies included immunohistochemistry, FDG PET/CT scans, and serum analyses for chemokines and microRNAs.
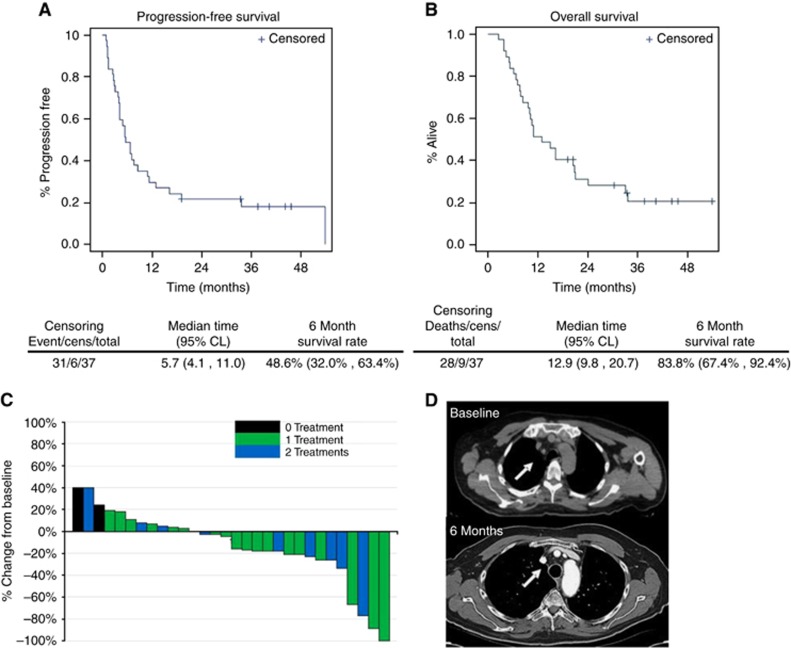
Thirty-six patients were enrolled, with 33 evaluable for toxicity and efficacy. Eighteen patients had 1 prior treatment, 13 patients had 2 prior treatments, and 2 patients were treatment naïve. Two patients experienced grade 4 thrombocytopenia and three patients had grade 3 thromboembolic events during the course of exposure. We observed six objective responses (18%), including one complete response and five partial responses. The proportion of patients with PFS at 6 months was 48%. The median PFS and overall survival were 5.7 months (confidence interval (CI): 4.1-11.0) and 13.9 months (CI: 9.8-20.7), respectively. Correlative studies showed that modulation of specific chemokines and microRNAs were associated with clinical benefit.
The combination of vorinostat with bevacizumab as described is relatively well tolerated. Response rate and median PFS suggest clinical activity for this combination strategy in previously treated ccRCC.
II类组蛋白去乙酰化酶(HDAC)抑制剂可诱导缺氧诱导因子-1和-2α降解,并与血管内皮生长因子(VEGF)抑制剂联合使用时具有抗肿瘤作用。在本研究中,我们测试了HDAC抑制剂伏立诺他和VEGF阻滞剂贝伐单抗在先前接受过包括舒尼替尼、索拉非尼、阿昔替尼、白细胞介素-2、干扰素和替西罗莫司等不同药物治疗的转移性透明细胞肾细胞癌(ccRCC)患者中的安全性和疗效。
接受过最多两种先前治疗方案的患者符合治疗条件,治疗方案为伏立诺他200mg口服,每日两次,共2周,以及贝伐单抗15mg/kg静脉注射,每3周一次。主要终点为安全性和耐受性,以及无进展生存期(PFS)达6个月的患者比例。相关研究包括免疫组织化学、FDG PET/CT扫描以及趋化因子和微小RNA的血清分析。
共纳入36例患者,其中33例可评估毒性和疗效。18例患者接受过1次先前治疗,13例患者接受过2次先前治疗,2例患者未曾接受过治疗。在治疗期间,2例患者出现4级血小板减少,3例患者出现3级血栓栓塞事件。我们观察到6例客观缓解(18%),包括1例完全缓解和5例部分缓解。6个月时PFS患者的比例为48%。PFS中位数和总生存期分别为5.7个月(置信区间(CI):4.1-11.0)和13.9个月(CI:9.8-20.7)。相关研究表明,特定趋化因子和微小RNA的调节与临床获益相关。
所述伏立诺他与贝伐单抗的联合方案耐受性相对良好。缓解率和PFS中位数表明该联合策略在先前治疗的ccRCC中具有临床活性。