Schindler Tim, Koller-Smith Louise, Lui Kei, Bajuk Barbara, Bolisetty Srinivas
Faculty of Medicine, University of New South Wales, Sydney, Australia.
Department of Newborn Care, Royal Hospital for Women, Sydney, Australia.
BMC Pediatr. 2017 Feb 21;17(1):59. doi: 10.1186/s12887-017-0810-3.
While there are good data to describe changing trends in mortality and morbidity rates for preterm populations, there is very little information on the specific causes and pattern of death in terms of age of vulnerability. It is well established that mortality increases with decreasing gestational age but there are limited data on the specific causes that account for this increased mortality. The aim of this study was to establish the common causes of hospital mortality in a regional preterm population admitted to a neonatal intensive care unit (NICU).
Retrospective analysis of prospectively collected data of the Neonatal Intensive Care Units' (NICUS) Data Collection of all 10 NICUs in the region. Infants <32 weeks gestation without major congenital anomalies admitted from 2007 to 2011 were included. Three authors reviewed all cases to agree upon the immediate cause of death.
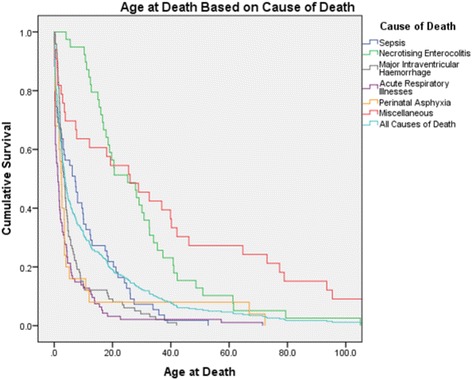
There were 345 (7.7%) deaths out of 4454 infants. The most common cause of death across all gestational groups was major IVH (cause-specific mortality rate [CMR] 22 per 1000 infants), followed by acute respiratory illnesses [ARI] (CMR 21 per 1000 infants) and sepsis (CMR 12 per 1000 infants). The most common cause of death was different in each gestational group (22-25 weeks [ARI], 26-28 weeks [IVH] and 29-31 weeks [perinatal asphyxia]). Pregnancy induced hypertension, antenatal steroids and chorioamnionitis were all associated with changes in CMRs. Deaths due to ARI or major IVH were more likely to occur at an earlier age (median [quartiles] 1.4 [0.3-4.4] and 3.6 [1.9-6.6] days respectively) in comparison to NEC and miscellaneous causes (25.2 [15.4-37.3] and 25.8 [3.2-68.9] days respectively).
Major IVH and ARI were the most common causes of hospital mortality in this extreme to very preterm population. Perinatal factors have a significant impact on cause-specific mortality. The varying timing of death provides insight into the prolonged vulnerability for diseases such as necrotising enterocolitis in our preterm population.
虽然有充分的数据描述早产人群死亡率和发病率的变化趋势,但关于脆弱期年龄方面的具体死因和死亡模式的信息却非常少。众所周知,死亡率随着孕周的减少而增加,但关于导致这种死亡率增加的具体原因的数据有限。本研究的目的是确定入住新生儿重症监护病房(NICU)的区域早产人群医院死亡的常见原因。
对该地区所有10个新生儿重症监护病房(NICUs)前瞻性收集的数据进行回顾性分析。纳入2007年至2011年收治的孕周小于32周且无重大先天性异常的婴儿。三位作者审查了所有病例,以就直接死因达成一致。
4454名婴儿中有345例(7.7%)死亡。所有孕周组中最常见的死因是重度脑室内出血(特定病因死亡率[CMR]为每1000名婴儿22例),其次是急性呼吸道疾病[ARI](CMR为每1000名婴儿21例)和败血症(CMR为每1000名婴儿12例)。每个孕周组中最常见的死因各不相同(22 - 25周[ARI]、26 - 28周[脑室内出血]和29 - 31周[围产期窒息])。妊娠高血压、产前类固醇和绒毛膜羊膜炎均与特定病因死亡率的变化有关。与坏死性小肠结肠炎和其他原因相比,ARI或重度脑室内出血导致的死亡更可能发生在较早年龄(中位数[四分位数]分别为1.4[0.3 - 4.4]天和3.6[1.9 - 6.6]天,而坏死性小肠结肠炎和其他原因分别为25.2[15.4 - 37.3]天和25.8[3.2 - 68.9]天)。
在这个极早产至非常早产的人群中,重度脑室内出血和ARI是医院死亡的最常见原因。围产期因素对特定病因死亡率有重大影响。死亡时间的差异为我们早产人群中坏死性小肠结肠炎等疾病的长期易感性提供了见解。