Schnabel Renate B, Pecen Ladislav, Ojeda Francisco M, Lucerna Markus, Rzayeva Nargiz, Blankenberg Stefan, Darius Harald, Kotecha Dipak, Caterina Raffaele De, Kirchhof Paulus
Department of Cardiology, University Heart Center Hamburg-Eppendorf, German Center for Cardiovascular Research (DZHK) partner site Hamburg/Kiel/Lübeck, Hamburg, Germany.
Medical Facility Pilsen of Charles University, Pilsen, Czech Republic.
Heart. 2017 Jul;103(13):1024-1030. doi: 10.1136/heartjnl-2016-310406. Epub 2017 Feb 22.
Our objective was to examine gender differences in clinical presentation, management and prognosis of atrial fibrillation (AF) in a contemporary cohort.
In 6412 patients, 39.7% women, of the PREvention oF thromboembolic events - European Registry in Atrial Fibrillation, we examined gender differences in symptoms, risk factors, therapies and 1-year incidence of adverse outcomes.
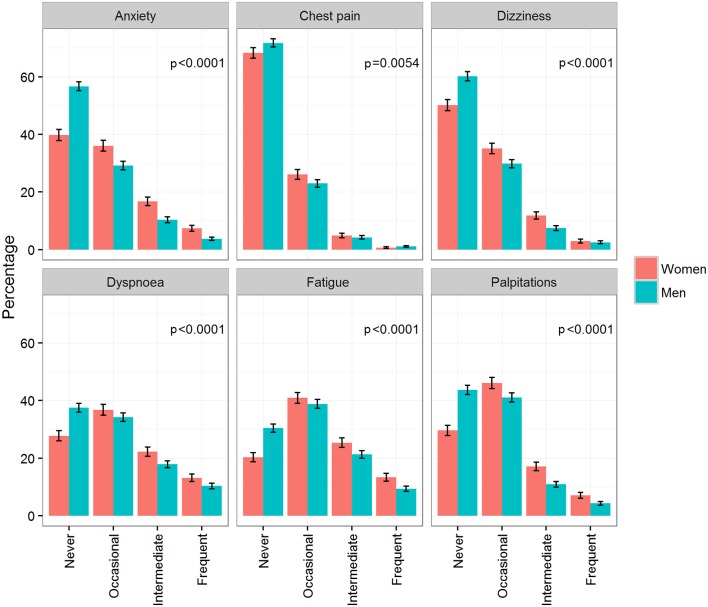
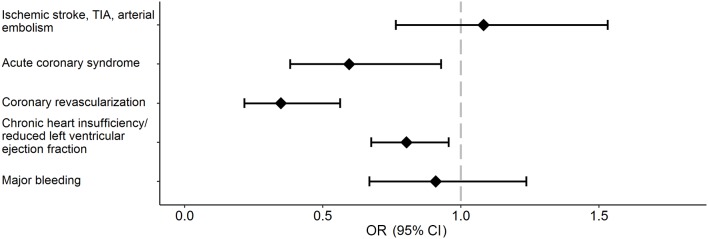
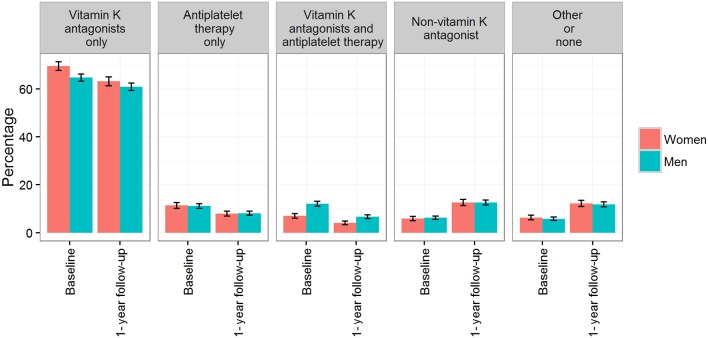
Men with AF were on average younger than women (mean±SD: 70.1±10.7 vs 74.1±9.7 years, p<0.0001). Women more frequently had at least one AF-related symptom at least occasionally compared with men (95.4% in women, 89.8% in men, p<0.0001). Prescription of oral anticoagulation was similar, with an increase of non-vitamin K antagonist oral anticoagulants from 5.9% to 12.6% in women and from 6.2% to 12.6% in men, p<0.0001 for both.Men were more frequently treated with electrical cardioversion and ablation (20.6% and 6.3%, respectively) than women (14.9% and 3.3%, respectively), p<0.0001. Women had 65% (OR: 0.35; 95% CI (0.22 to 0.56)) lower age-adjusted and country-adjusted odds of coronary revascularisation, 40% (OR: 0.60; (0.38 to 0.93)) lower odds of acute coronary syndrome and 20% (OR: 0.80; (0.68 to 0.96)) lower odds of heart failure at 1 year. There were no statistically significant gender differences in 1-year stroke/transient ischaemic attack/arterial thromboembolism and major bleeding events.
In a 'real-world' European AF registry, women were more symptomatic but less likely to receive invasive rhythm control therapy such as electrical cardioversion or ablation. Further study is needed to confirm that these differences do not disadvantage women with AF.
我们的目的是在一个当代队列中研究心房颤动(AF)临床表现、治疗及预后方面的性别差异。
在预防血栓栓塞事件——欧洲心房颤动注册研究的6412例患者中,女性占39.7%,我们研究了症状、危险因素、治疗方法及不良结局1年发生率方面的性别差异。
房颤男性患者的平均年龄低于女性(均值±标准差:70.1±10.7岁对74.1±9.7岁,p<0.0001)。与男性相比,女性更频繁地至少偶尔出现一种与房颤相关的症状(女性为95.4%,男性为89.8%,p<0.0001)。口服抗凝药的处方情况相似,女性中新型口服抗凝药的使用比例从5.9%增至12.6%,男性从6.2%增至12.6%,二者均p<0.0001。男性接受电复律和消融治疗的频率高于女性(分别为20.6%和6.3%)(女性分别为14.9%和3.3%),p<0.0001。校正年龄和国家后,女性进行冠状动脉血运重建的几率低65%(比值比:0.35;95%置信区间(0.22至0.56)),急性冠状动脉综合征的几率低40%(比值比:0.60;(0.38至0.93)),1年时发生心力衰竭的几率低20%(比值比:0.80;(0.68至0.96))。在1年的卒中/短暂性脑缺血发作/动脉血栓栓塞和大出血事件方面,性别差异无统计学意义。
在一项“真实世界”的欧洲房颤注册研究中,女性症状更多,但接受侵入性节律控制治疗(如电复律或消融)的可能性较小。需要进一步研究以证实这些差异不会对房颤女性患者不利。