3rd Medical Department, Cardiology and Intensive Care Medicine, Wilhelminen Hospital, Vienna, Austria.
Institute for Cardiometabolic Diseases, Karl Landsteiner Society, St. Pölten, Austria.
BMJ Open. 2019 Mar 30;9(3):e022478. doi: 10.1136/bmjopen-2018-022478.
We identified factors associated with thromboembolic and bleeding events in two contemporary cohorts of anticoagulated patients with atrial fibrillation (AF), treated with either vitamin K antagonists (VKA) or non-VKA oral anticoagulants (NOACs).
Prospective, multicentre observational study.
461 centres in seven European countries.
5310 patients receiving a VKA (PREvention oF thromboembolic events - European Registry in Atrial Fibrillation (PREFER in AF), derivation cohort) and 3156 patients receiving a NOAC (PREFER in AF Prolongation, validation cohort) for stroke prevention in AF.
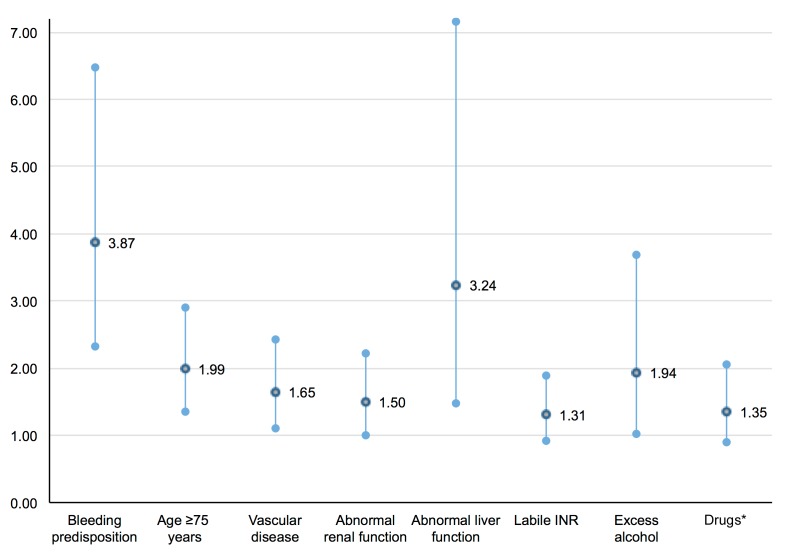
Risk factors for thromboembolic events (ischaemic stroke, systemic embolism) and major bleeding (gastrointestinal bleeding, intracerebral haemorrhage and other life-threatening bleeding).
The mean age of patients enrolled in the PREFER in AF registry was 72±10 years, 40% were female and the mean CHADS-VASc Score was 3.5±1.7. The incidence of thromboembolic and major bleeding events was 2.34% (95% CI 1.93% to 2.74%) and 2.84% (95% CI 2.41% to 3.33%) after 1-year of follow-up, respectively.Abnormal liver function, prior stroke or transient ischaemic attack, labile international normalised ratio (INR), concomitant therapy with antiplatelet or non-steroidal anti-inflammatory drugs, heart failure and older age (≥75 years) were independently associated with both thromboembolic and major bleeding events.With the exception of unstable INR values, these risk factors were validated in patients treated with NOACs (PREFER in AF Prolongation Study, 72±9 years, 40% female, CHADS-VASc 3.3±1.6). For each single point decrease on a modifiable bleeding risk scale we observed a 30% lower risk for major bleeding events (OR 0.70, 95% CI 0.64 to 0.76, p<0.01) and a 28% lower rate of thromboembolic events (OR 0.72, 95% CI 0.66 to 0.82, p<0.01).
Attending to modifiable risk factors is an important treatment target in anticoagulated AF patients to reduce thromboembolic and bleeding events. Initiation of anticoagulation in those at risk of stroke should not be prevented by elevated bleeding risk scores.
我们在两个当代抗凝心房颤动(AF)患者队列中确定了与血栓栓塞和出血事件相关的因素,这些患者分别接受维生素 K 拮抗剂(VKA)或非 VKA 口服抗凝剂(NOAC)治疗。
前瞻性、多中心观察性研究。
欧洲 7 个国家的 461 个中心。
5310 例接受 VKA(预防血栓栓塞事件-心房颤动欧洲登记处(PREFER in AF),推导队列)和 3156 例接受 NOAC(PREFER in AF 延长,验证队列)治疗的 AF 患者用于预防卒中。
血栓栓塞事件(缺血性中风、全身性栓塞)和大出血(胃肠道出血、颅内出血和其他危及生命的出血)的危险因素。
纳入 PREFER in AF 登记处的患者平均年龄为 72±10 岁,40%为女性,平均 CHADS-VASc 评分为 3.5±1.7。随访 1 年后,血栓栓塞和大出血事件的发生率分别为 2.34%(95%CI 1.93%至 2.74%)和 2.84%(95%CI 2.41%至 3.33%)。肝功能异常、既往卒中和短暂性脑缺血发作、不稳定的国际标准化比值(INR)、同时接受抗血小板或非甾体抗炎药治疗、心力衰竭和年龄较大(≥75 岁)与血栓栓塞和大出血事件均独立相关。除不稳定的 INR 值外,这些危险因素在接受 NOAC 治疗的患者中得到了验证(PREFER in AF 延长研究,72±9 岁,40%为女性,CHADS-VASc 为 3.3±1.6)。对于可改变的出血风险评分每降低一个点,大出血事件的风险降低 30%(OR 0.70,95%CI 0.64 至 0.76,p<0.01),血栓栓塞事件的发生率降低 28%(OR 0.72,95%CI 0.66 至 0.82,p<0.01)。
关注可改变的危险因素是抗凝 AF 患者减少血栓栓塞和出血事件的重要治疗目标。升高的出血风险评分不应阻止高危卒中患者开始抗凝治疗。