Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Lancet Diabetes Endocrinol. 2017 Apr;5(4):271-279. doi: 10.1016/S2213-8587(17)30061-X. Epub 2017 Feb 23.
Bariatric surgery is associated with remission of diabetes and prevention of diabetic complications in patients with obesity and type 2 diabetes. Long-term effects of bariatric surgery on microvascular complications in patients with prediabetes are unknown. The aim of this study was to examine the effects of bariatric surgery on incidence of microvascular complications in patients with obesity stratified by baseline glycaemic status.
Patients were recruited to the Swedish Obese Subjects (SOS) study between Sept 1, 1987, and Jan 31, 2001. Inclusion criteria were age 37-60 years and BMI of 34 kg/m or greater in men and 38 kg/m or greater in women. Exclusion criteria were identical in surgery and control groups and designed to exclude patients not suitable for surgery. The surgery group (n=2010) underwent gastric bypass (265 [13%]), gastric banding (376 [19%]), or vertical-banded gastroplasty (1369 [68%]). Participants in the control group (n=2037) received usual care. Bodyweight was measured and questionnaires were completed at baseline and at 0·5 years, 1 year, 2 years, 3 years, 4 years, 6 years, 8 years, 10 years, 15 years, and 20 years. Biochemical variables were measured at baseline and at 2 years, 10 years, and 15 years. We categorised participants into subgroups on the basis of baseline glycaemic status (normal [fasting blood glucose concentration <5·0 mmol/L], prediabetes [5·0-6·0 mmol/L], screen-detected diabetes [≥6·1 mmol/L at baseline visit without previous diagnosis], and established diabetes [diagnosis of diabetes before study inclusion]). We obtained data about first incidence of microvascular disease from nationwide registers and about diabetes incidence at study visits at 2 years, 10 years, and 15 years. We did the main analysis by intention to treat, and subgroup analyses after stratification by baseline glycaemic status and by diabetes status at the 15 year follow-up. The SOS study is registered with ClinicalTrials.gov, NCT01479452.
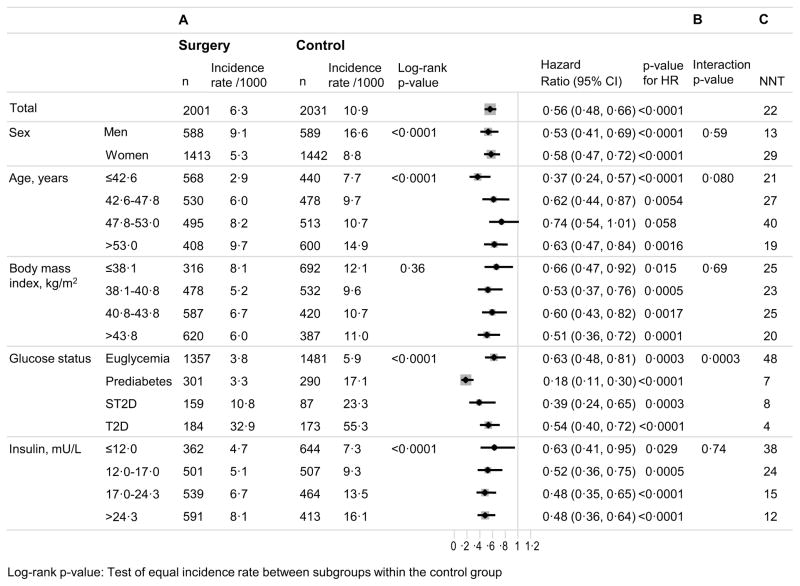
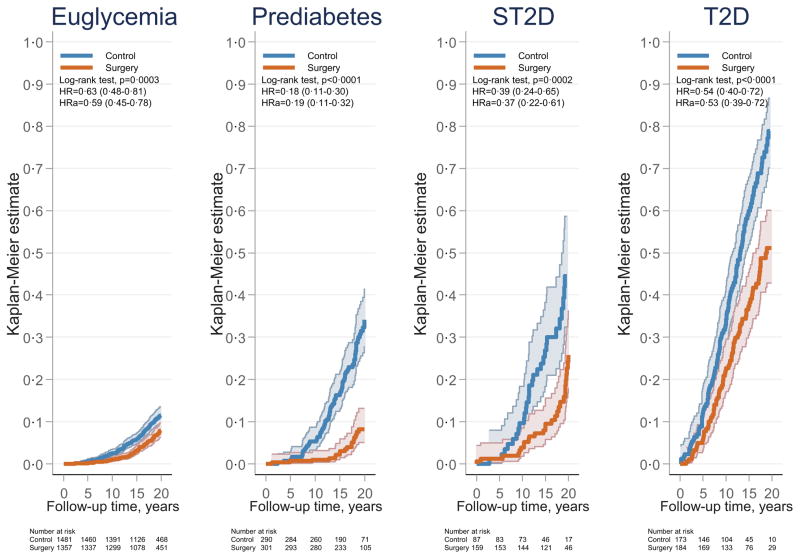
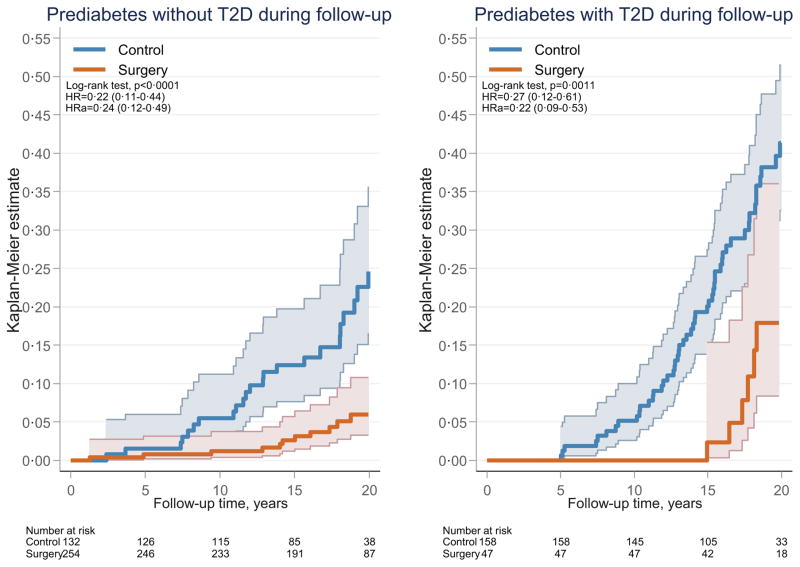
4032 of the 4047 participants in the SOS study were included in this analysis. We excluded four patients with suspected type 1 diabetes, and 11 patients with unknown glycaemic status at baseline. At baseline, 2838 patients had normal blood glucose, 591 had prediabetes, 246 had screen-detected diabetes, and 357 had established diabetes. Median follow-up was 19 years (IQR 16-21). We identified 374 incident cases of microvascular disease in the control group and 224 in the surgery group (hazard ratio [HR] 0·56, 95% CI 0·48-0·66; p<0·0001). Interaction between baseline glycaemic status and effect of treatment on incidence of microvascular disease was significant (p=0·0003). Unadjusted HRs were lowest in the subgroup with prediabetes (0·18, 95% CI 0·11-0·30), followed by subgroups with screen-detected diabetes (0·39, 0·24-0·65), established diabetes (0·54, 0·40-0·72), and normoglycaemia (0·63, 0·48-0·81). Surgery was associated with reduced incidence of microvascular events in people with prediabetes regardless of whether they developed diabetes during follow-up.
Bariatric surgery was associated with reduced risk of microvascular complications in all subgroups, but the greatest relative risk reduction was observed in patients with prediabetes at baseline. Our results suggest that prediabetes should be treated aggressively to prevent future microvascular events, and effective non-surgical treatments need to be developed for this purpose.
US National Institutes of Health, Swedish Research Council, Sahlgrenska University Hospital Regional Agreement on Medical Education and Research, and Swedish Diabetes Foundation.
减重手术可使肥胖合并 2 型糖尿病患者的糖尿病缓解并预防糖尿病并发症。对于糖尿病前期患者,减重手术对微血管并发症的长期影响尚不清楚。本研究旨在检查在不同基线血糖状态下,减重手术对肥胖患者微血管并发症发生率的影响。
患者于 1987 年 9 月 1 日至 2001 年 1 月 31 日被纳入瑞典肥胖受试者(SOS)研究。纳入标准为年龄 37-60 岁,男性 BMI 为 34kg/m2 或以上,女性 BMI 为 38kg/m2 或以上。手术组(n=2010)接受胃旁路术(265[13%])、胃束带术(376[19%])或垂直带胃成形术(1369[68%])。对照组(n=2037)接受常规护理。参与者在基线和 0.5 年、1 年、2 年、3 年、4 年、6 年、8 年、10 年、15 年和 20 年进行体重测量和问卷调查。生化变量在基线和 2 年、10 年和 15 年进行测量。我们根据基线血糖状态(空腹血糖浓度<5.0mmol/L[正常]、5.0-6.0mmol/L[糖尿病前期]、基线就诊时检出的糖尿病[≥6.1mmol/L 而无先前诊断]和确诊的糖尿病[研究纳入前诊断的糖尿病])将参与者分为亚组。我们从全国登记处获得微血管疾病首次发病的数据,并在基线、2 年、10 年和 15 年随访时通过研究就诊获得糖尿病发病数据。我们通过意向治疗进行主要分析,并在基线血糖状态和 15 年随访时的糖尿病状态分层后进行亚组分析。SOS 研究在 ClinicalTrials.gov 上注册,NCT01479452。
在 SOS 研究的 4047 名参与者中,有 4032 名符合纳入标准。我们排除了 4 名疑似 1 型糖尿病患者和 11 名基线血糖状态未知的患者。基线时,2838 名患者血糖正常,591 名患者糖尿病前期,246 名患者筛查出糖尿病,357 名患者确诊糖尿病。中位随访时间为 19 年(IQR 16-21)。在对照组中,我们发现 374 例微血管疾病新发病例,手术组中发现 224 例(风险比[HR]0.56,95%CI 0.48-0.66;p<0.0001)。治疗对微血管疾病发病率的影响与基线血糖状态之间的交互作用有统计学意义(p=0.0003)。未调整的 HR 在糖尿病前期亚组中最低(0.18,95%CI 0.11-0.30),随后依次为筛查出的糖尿病亚组(0.39,0.24-0.65)、确诊的糖尿病亚组(0.54,0.40-0.72)和血糖正常亚组(0.63,0.48-0.81)。无论患者在随访期间是否发生糖尿病,减重手术都与微血管事件发生率降低相关。
减重手术可降低所有亚组的微血管并发症风险,但在基线时患有糖尿病前期的患者中,相对风险降低幅度最大。我们的研究结果表明,应积极治疗糖尿病前期以预防未来的微血管事件,并为此目的开发有效的非手术治疗方法。
美国国立卫生研究院、瑞典研究委员会、萨赫勒格伦斯卡大学医院区域医学教育和研究协议以及瑞典糖尿病基金会。