Huber Thomas, Alber Georgina, Bette Stefanie, Kaesmacher Johannes, Boeckh-Behrens Tobias, Gempt Jens, Ringel Florian, Specht Hanno M, Meyer Bernhard, Zimmer Claus, Wiestler Benedikt, Kirschke Jan S
Department of Neuroradiology, Klinikum rechts der Isar, Technical University of Munich, Germany.
Institute for Clinical Radiology, Ludwig-Maximilians-University Hospital, Munich, Germany.
PLoS One. 2017 Feb 28;12(2):e0173112. doi: 10.1371/journal.pone.0173112. eCollection 2017.
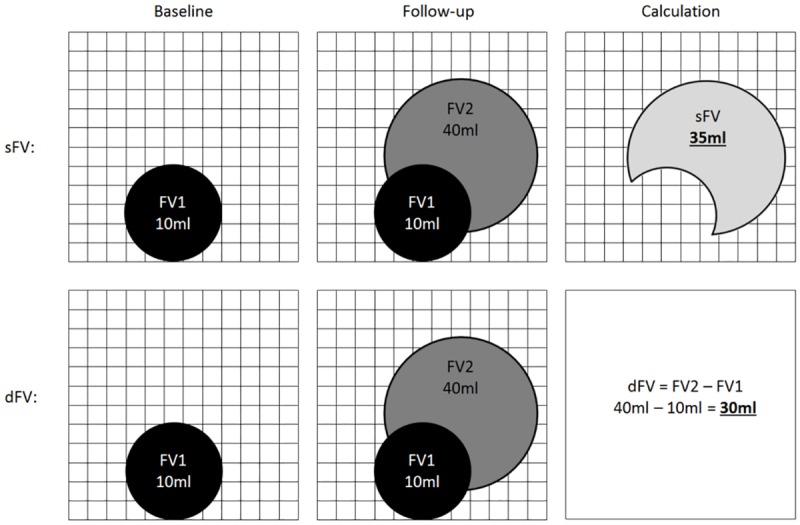
Unambiguous evaluation of glioblastoma (GB) progression is crucial, both for clinical trials as well as day by day routine management of GB patients. 3D-volumetry in the follow-up of GB provides quantitative data on tumor extent and growth, and therefore has the potential to facilitate objective disease assessment. The present study investigated the utility of absolute changes in volume (delta) or regional, segmentation-based subtractions for detecting disease progression in longitudinal MRI follow-ups.
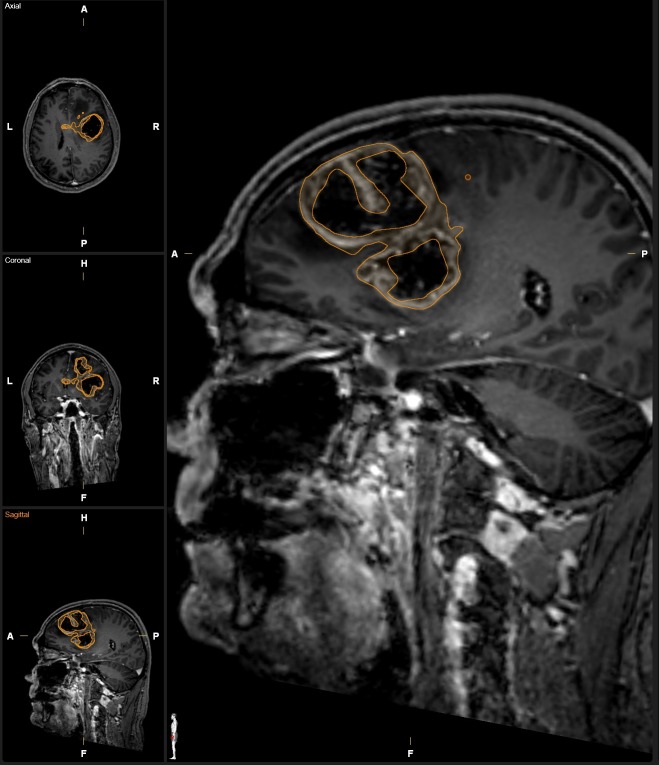
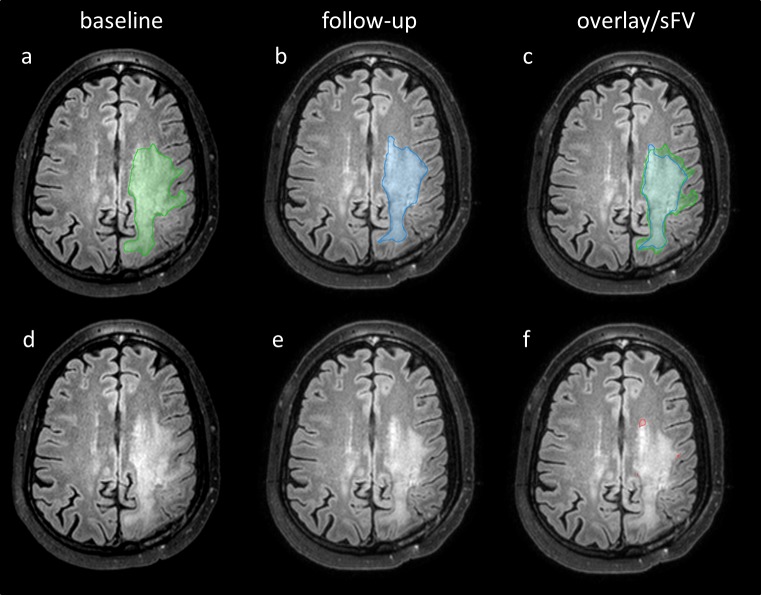
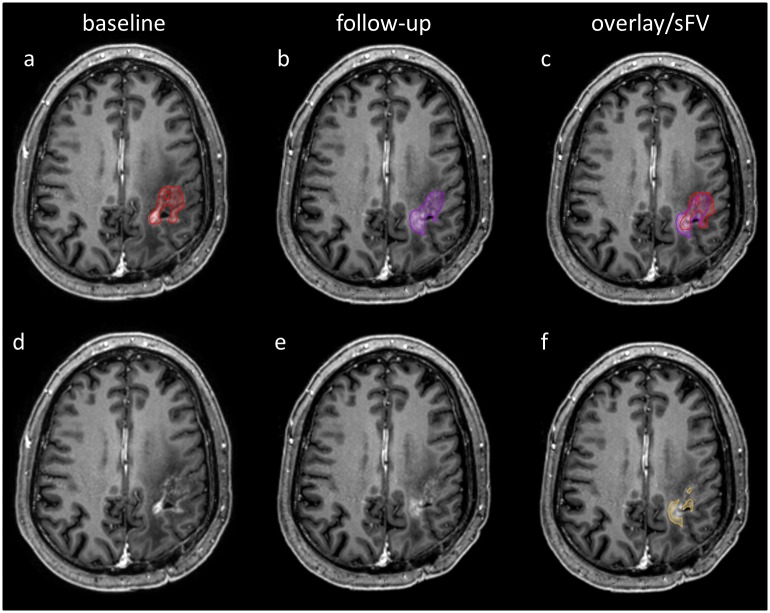
165 high resolution 3-Tesla MRIs of 30 GB patients (23m, mean age 60.2y) were retrospectively included in this single center study. Contrast enhancement (CV) and tumor-related signal alterations in FLAIR images (FV) were semi-automatically segmented. Delta volume (dCV, dFV) and regional subtractions (sCV, sFV) were calculated. Disease progression was classified for every follow-up according to histopathologic results, decisions of the local multidisciplinary CNS tumor board and a consensus rating of the neuro-radiologic report.
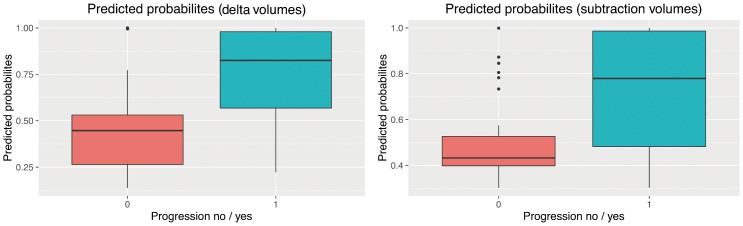
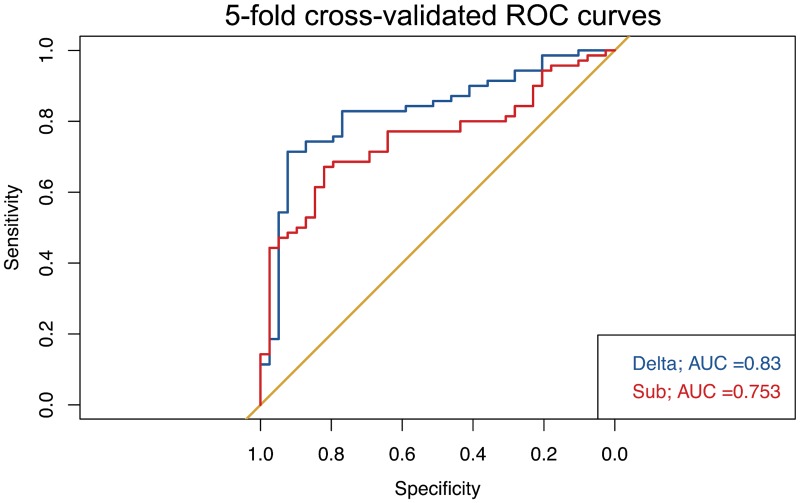
A generalized logistic mixed model for disease progression (yes / no) with dCV, dFV, sCV and sFV as input variables revealed that only dCV was significantly associated with prediction of disease progression (P = .005). Delta volume had a better accuracy than regional, segmentation-based subtractions (79% versus 72%) and a higher area under the curve by trend in ROC curves (.83 versus .75).
Absolute volume changes of the contrast enhancing tumor part were the most accurate volumetric determinant to detect progressive disease in assessment of GB and outweighed FLAIR changes as well as regional, segmentation-based image subtractions. This parameter might be useful in upcoming objective response criteria for glioblastoma.
准确评估胶质母细胞瘤(GB)的进展情况至关重要,这对于临床试验以及GB患者的日常常规管理均是如此。GB随访中的三维容积测量可提供有关肿瘤范围和生长的定量数据,因此有潜力促进客观的疾病评估。本研究调查了体积的绝对变化(增量)或基于区域分割的减法在纵向MRI随访中检测疾病进展的效用。
本单中心研究回顾性纳入了30例GB患者(23名男性,平均年龄60.2岁)的165份高分辨率3特斯拉MRI图像。对对比增强(CV)和液体衰减反转恢复(FLAIR)图像中的肿瘤相关信号改变(FV)进行半自动分割。计算增量体积(dCV、dFV)和区域减法(sCV、sFV)。根据组织病理学结果、当地多学科中枢神经系统肿瘤委员会的决定以及神经放射学报告的共识评级,对每次随访的疾病进展进行分类。
以dCV、dFV、sCV和sFV作为输入变量的疾病进展(是/否)广义逻辑混合模型显示,只有dCV与疾病进展预测显著相关(P = 0.005)。增量体积比基于区域分割的减法具有更高的准确性(79%对72%),并且在ROC曲线中的曲线下面积趋势更高(0.83对0.75)。
在评估GB时,对比增强肿瘤部分的绝对体积变化是检测疾病进展最准确的数据决定因素,其优于FLAIR变化以及基于区域分割的图像减法。该参数可能对即将出台的胶质母细胞瘤客观反应标准有用。