Sammani A, Wind A M, Kirkels J H, Klöpping C, Buijsrogge M P, Ramjakhan F Z, Asselbergs F W, de Jonge N
Department of Cardiology, UMC Utrecht, Utrecht, The Netherlands.
Department of Cardiothoracic Surgery, UMC Utrecht, Utrecht, The Netherlands.
Neth Heart J. 2017 Sep;25(9):516-523. doi: 10.1007/s12471-017-0969-0.
To analyse patient demographics, indications, survival and donor characteristics for heart transplantation (HTx) during the past 30 years at the University Medical Centre Utrecht (UMCU).
Data have been prospectively collected for all patients who underwent HTx at the UMCU from 1985 until 2015. Patients who were included underwent orthotopic HTx at an age >14 years.
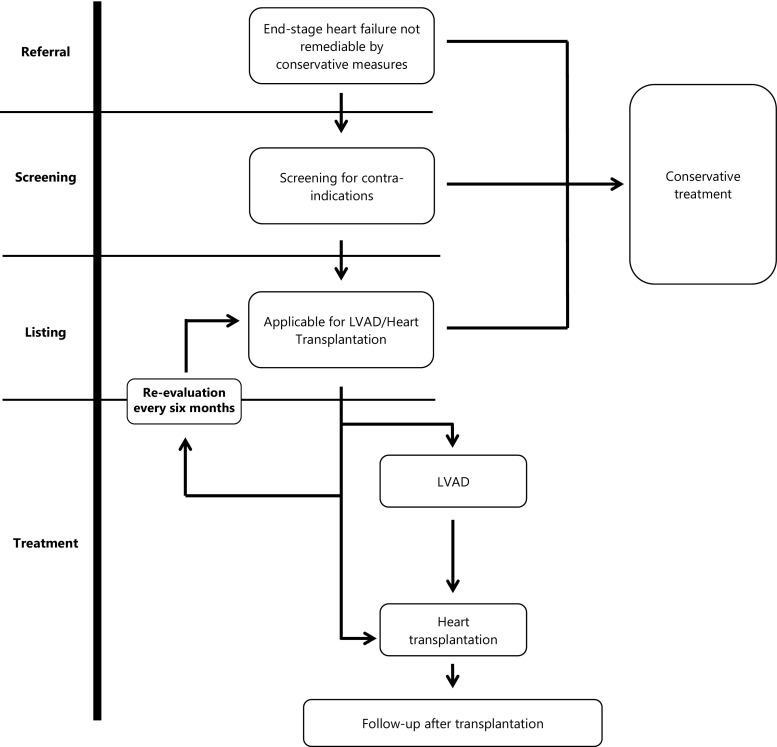
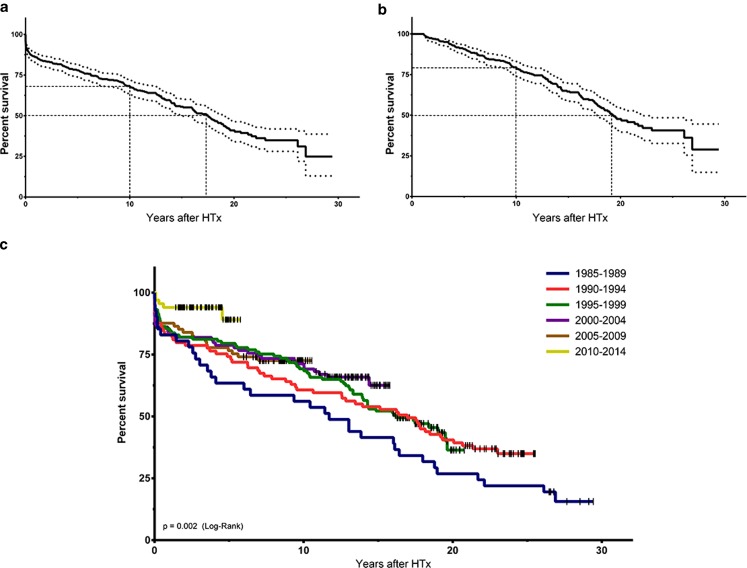
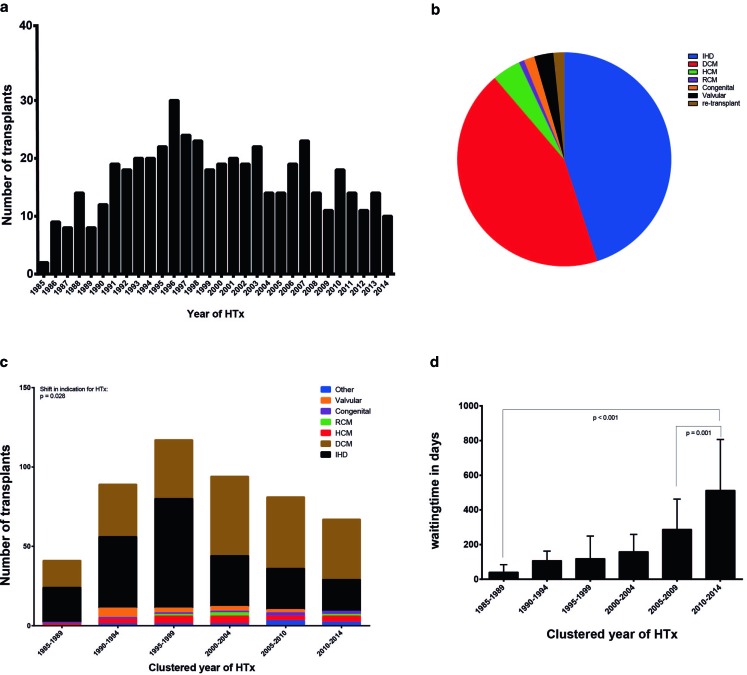
In total, 489 hearts have been transplanted since 1985; 120 patients (25%) had left ventricular assist device (LVAD) implantation prior to HTx. A shift from ischaemic heart disease to dilated cardiomyopathy has been seen as the leading indication for HTx since the year 2000. Median age at HTx was 49 years (range 16-68). Median waiting time and donor age have also increased from 40 to 513 days and from 27 to 44 years respectively (range 11-65). Donor cause of death is now primarily stroke, in contrast to head and brain injury in earlier years. Estimated median survival is 15.4 years (95% confidence interval 14.2-16.6) There is better survival throughout these years.
Over the past 30 years, patient and donor demographics and underlying diseases have shifted substantially. Furthermore, the increase in waiting time due to lack of available donor hearts has led to a rise in the use of LVADs as bridge to transplant. Importantly, an improvement in survival rates is found over time which could be explained by better immunosuppressive therapy and improvements in follow-up care.
分析乌得勒支大学医学中心(UMCU)过去30年心脏移植(HTx)患者的人口统计学特征、适应证、生存率及供体特征。
前瞻性收集了1985年至2015年在UMCU接受HTx的所有患者的数据。纳入的患者年龄>14岁,接受原位心脏移植。
自1985年以来,共进行了489例心脏移植;120例患者(25%)在HTx前植入了左心室辅助装置(LVAD)。自2000年以来,HTx的主要适应证已从缺血性心脏病转变为扩张型心肌病。HTx时的中位年龄为49岁(范围16 - 68岁)。中位等待时间和供体年龄也分别从40天增加到513天,从27岁增加到44岁(范围11 - 65岁)。与早年主要是头部和脑损伤不同,目前供体的死亡原因主要是中风。估计中位生存期为15.4年(95%置信区间14.2 - 16.6),这些年的生存率有所提高。
在过去30年中,患者和供体的人口统计学特征及基础疾病发生了显著变化。此外,由于可用供体心脏短缺导致等待时间增加,促使LVAD作为移植桥梁的使用增加。重要的是,随着时间推移发现生存率有所提高,这可能归因于更好的免疫抑制治疗和随访护理的改善。