Serbanescu G L, Anghel R M
Prof. Dr. Al. Trestioreanu" Institute of Oncology, Bucharest, Romania.
"Carol Davila'' University of Medicine and Pharmacy, Bucharest, Romania.
J Med Life. 2017 Jan-Mar;10(1):66-69.
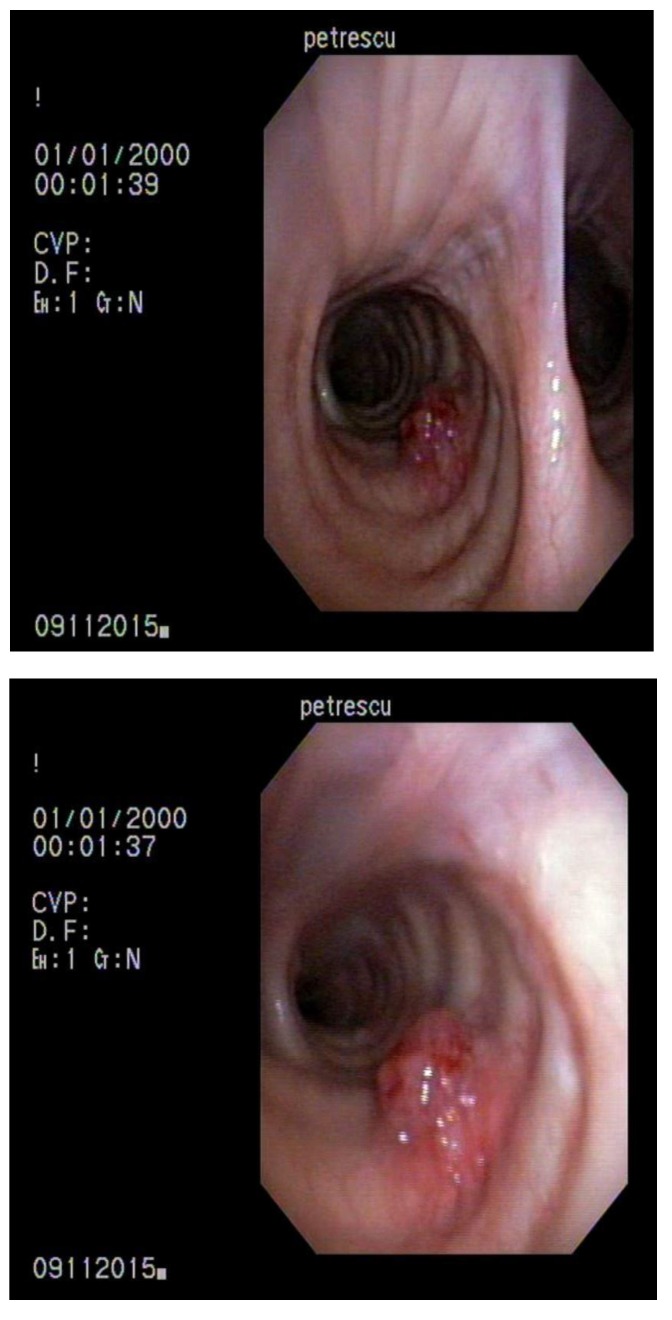
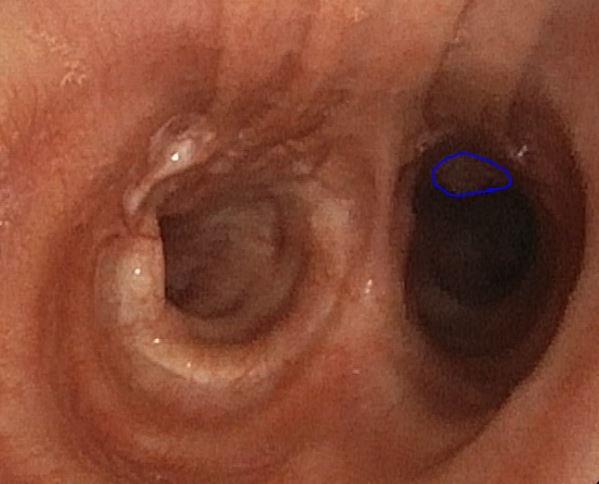
Endobronchial and endotracheal metastases from extra-pulmonary solid tumors are rare. We reported the case of a patient diagnosed with endobronchial and endotracheal metastases from rectal adenocarcinoma. Patient P.G., 62 years old, was diagnosed with a rectal tumor in 2011, for which, a surgical intervention was performed (pT3 pN2a M0, stage IIIB). Afterwards, she underwent adjuvant chemotherapy and concomitant radiochemotherapy. In September 2013, the chest CT showed 2 nodules for which, an incomplete surgical resection was done and which were histopathologically diagnosed as metastases from rectal cancer. The patient continued the treatment with chemotherapy associated with Bevacizumab and after 6 months only Bevacizumab for maintenance. In June 2015, the chest CT pointed out a nodule in the right upper lobe and the bronchoscopy highlighted a 4-5 mm lesion at the level of the right primary bronchus, whose biopsy proved the rectal origin. Afterwards, another surgical intervention was performed. Unfortunately, the postoperative chest CT revealed an intratracheal tissue mass (11/ 7mm) and multiple metastases in the right lung. The bronchoscopy showed 2 endotracheal lesions, out of which one was biopsied (histopathological result of metastasis from rectal cancer). Despite the fact that chemotherapy was continued, other endobronchial lesions appeared. All of them were removed and the patient started radiotherapy on the tracheal area. Afterwards, she refused to continue chemotherapy. The last bronchoscopy highlighted one endobronchial and two endotracheal secondary malignant lesions. Endobronchial and endotracheal metastases must be taken into consideration in all the patients with a history of extra-pulmonary cancer. CT = computed tomography, MRI = magnetic resonance imaging, IMRT = intensity-modulated radiotherapy, ESMO = European Society for Medical Oncology, NCCN = National Comprehensive Cancer Network, iv = intravenous, PET - CT = Positron Emission Tomography - Computed Tomography.
肺外实体瘤的支气管内和气管内转移罕见。我们报告了一例被诊断为直肠腺癌支气管内和气管内转移的患者。患者P.G.,62岁,2011年被诊断出患有直肠肿瘤,为此接受了手术干预(pT3 pN2a M0,IIIB期)。之后,她接受了辅助化疗和同步放化疗。2013年9月,胸部CT显示有2个结节,对其进行了不完全手术切除,组织病理学诊断为直肠癌转移。患者继续接受与贝伐单抗联合的化疗,6个月后仅用贝伐单抗维持治疗。2015年6月,胸部CT显示右上叶有一个结节,支气管镜检查发现右主支气管水平有一个4 - 5毫米的病变,活检证实为直肠来源。之后,进行了另一次手术干预。不幸的是,术后胸部CT显示气管内有一个组织块(11/7毫米)以及右肺多发转移。支气管镜检查显示有2个气管内病变,其中一个进行了活检(组织病理学结果为直肠癌转移)。尽管继续进行了化疗,但仍出现了其他支气管内病变。所有病变均被切除,患者开始对气管区域进行放疗。之后,她拒绝继续化疗。最后一次支气管镜检查发现一个支气管内和两个气管内继发性恶性病变。对于所有有肺外癌症病史的患者,都必须考虑支气管内和气管内转移。CT = 计算机断层扫描,MRI = 磁共振成像,IMRT = 调强放射治疗,ESMO = 欧洲医学肿瘤学会,NCCN = 美国国立综合癌症网络,iv = 静脉注射,PET - CT = 正电子发射断层扫描 - 计算机断层扫描