Fairley Lesley, Stark Daniel P, Yeomanson Daniel, Kinsey Sally E, Glaser Adam W, Picton Susan V, Evans Linda, Feltbower Richard G
Division of Epidemiology and Biostatistics, School of Medicine, Worsley Building, University of Leeds, Clarendon Way, Leeds, UK, LS2 9JT.
St James's Institute of Oncology, Leeds Institute of Cancer and Pathology, University of Leeds and Leeds Teaching Hospitals NHS Trust, Bexley Wing, St James's Hospital, Beckett Street, Leeds, LS9 7TF, UK.
BMC Cancer. 2017 Mar 4;17(1):168. doi: 10.1186/s12885-017-3160-5.
Principal Treatment Centres (PTC) were established to provide age-appropriate care as well as clinical expertise for children and young people with cancer. However, little is known about the effects of specialist treatment centres on survival outcomes especially for teenagers and young adults. This population-based study aimed to describe access to PTC and the associated trends in survival for 0-24 year olds accounting for stage of disease at presentation and treatment.
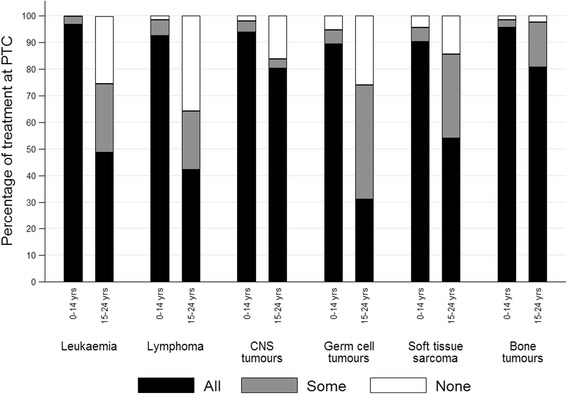
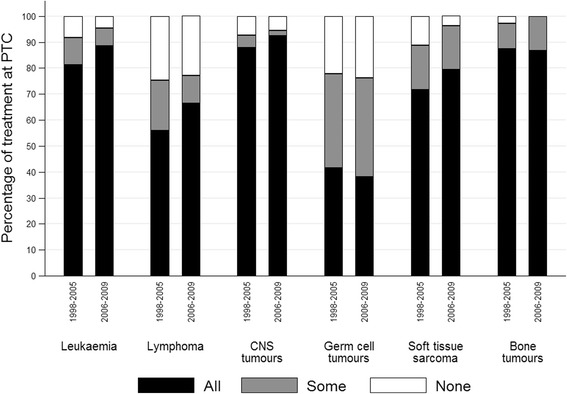
Patients diagnosed from 1998-2009 aged 0-24 years were extracted from the Yorkshire Specialist Register of Cancer in Children and Young People, including information on all treating hospitals, followed-up until 31st December 2014. The six commonest cancer types were included: leukaemia (n = 684), lymphoma (n = 558), CNS tumours (n = 547), germ cell tumours (n = 364), soft tissue sarcomas (n = 171) and bone tumours (n = 163). Treatment was categorised into three groups: 'all', 'some' or 'no' treatment received at a PTC. Treatment at PTC was examined by diagnostic group and patient characteristics. Overall survival was modelled using Cox regression adjusting for case-mix including stage, treatment and other socio-demographic and clinical characteristics.
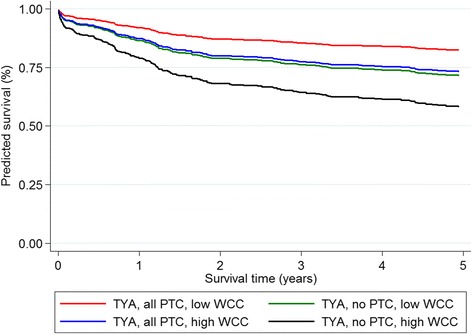
Overall 72% of patients received all their treatment at PTC whilst 13% had no treatment at PTC. This differed by diagnostic group and age at diagnosis. Leukaemia patients who received no treatment at PTC had an increased risk of death which was partially explained by differences in patient case-mix (adjusted Hazard Ratio (HR) = 1.73 (95%CI 0.98-3.04)). Soft tissue sarcoma patients who had some or no treatment at PTC had better survival outcomes, which remained after adjustment for patient case-mix (adjusted HR = 0.48 (95%CI 0.23-0.99)). There were no significant differences in outcomes for other diagnostic groups (lymphoma, CNS tumours, bone tumours and germ cell tumours). For leukaemia patients survival outcomes for low risk patients receiving no treatment at PTC were similar to high risk patients who received all treatment at PTC, implying a benefit for care at the PTC.
This study demonstrates that for leukaemia patients receiving treatment at a PTC is associated with improved survival that may compensate for a poorer prognosis presentation. However, further information on risk factors is needed for all diagnostic groups in order to fully account for differences in patient case-mix.
设立主要治疗中心(PTC)是为了为患癌儿童和青少年提供适合其年龄阶段的护理以及临床专业知识。然而,对于专科治疗中心对生存结果的影响知之甚少,尤其是对青少年和青年成人而言。这项基于人群的研究旨在描述0至24岁患者获得PTC治疗的情况以及与之相关的生存趋势,并考虑到就诊时的疾病阶段和治疗情况。
从约克郡儿童和青少年癌症专科登记册中提取1998年至2009年诊断的0至24岁患者,包括所有治疗医院的信息,随访至2014年12月31日。纳入六种最常见的癌症类型:白血病(n = 684)、淋巴瘤(n = 558)、中枢神经系统肿瘤(n = 547)、生殖细胞肿瘤(n = 364)、软组织肉瘤(n = 171)和骨肿瘤(n = 163)。治疗分为三组:在PTC接受“全部”、“部分”或“无”治疗。通过诊断组和患者特征来检查在PTC的治疗情况。使用Cox回归对总体生存进行建模,并对病例组合进行调整,包括疾病阶段、治疗以及其他社会人口统计学和临床特征。
总体而言,72%的患者在PTC接受了全部治疗,而13%的患者在PTC未接受任何治疗。这因诊断组和诊断时的年龄而异。在PTC未接受治疗的白血病患者死亡风险增加,部分原因可由患者病例组合的差异解释(调整后风险比(HR)= 1.73(95%置信区间0.98 - 3.04))。在PTC接受部分或未接受治疗的软组织肉瘤患者生存结果更好,在对患者病例组合进行调整后仍然如此(调整后HR = 0.48(95%置信区间0.23 - 0.99))。其他诊断组(淋巴瘤、中枢神经系统肿瘤、骨肿瘤和生殖细胞肿瘤)的结果没有显著差异。对于白血病患者,在PTC未接受治疗的低风险患者的生存结果与在PTC接受全部治疗的高风险患者相似,这意味着在PTC接受治疗有益。
这项研究表明,对于白血病患者,在PTC接受治疗与生存改善相关,这可能弥补预后较差的情况。然而,为了全面解释患者病例组合的差异,所有诊断组都需要更多关于风险因素的信息。