Boutin Robert D, Bamrungchart Sara, Bateni Cyrus P, Beavers Daniel P, Beavers Kristen M, Meehan John P, Lenchik Leon
1 Department of Radiology, University of California Davis School of Medicine, 4860 Y St, Ste 3100, Sacramento, CA 95817.
2 Department of Biostatistical Sciences, Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, NC.
AJR Am J Roentgenol. 2017 Jun;208(6):W208-W215. doi: 10.2214/AJR.16.17226. Epub 2017 Mar 7.
Our objective was to determine the association between muscle cross-sectional area and attenuation, as measured on routine CT scans, and mortality in older patients with hip fracture.
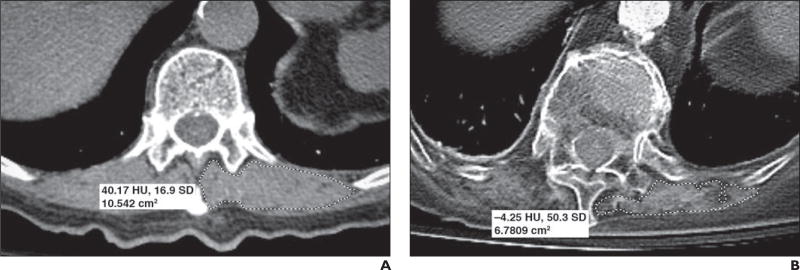
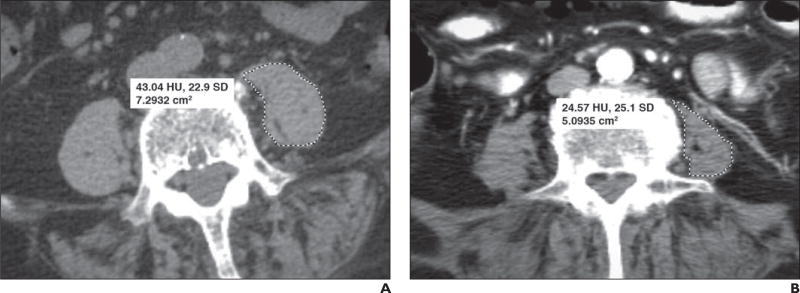
A retrospective 10-year study of patients with hip fracture was conducted with the following inclusion criteria: age 65 years or older, first-time hip fracture treated with surgery, and CT of the chest, abdomen, or pelvis. This yielded 274 patients (70.4% women; mean [± SD] age, 81.3 ± 8.3 years). On each CT scan, two readers independently measured the size (cross-sectional area, indexed for patient height) and attenuation of the paravertebral muscle at T12 and the psoas muscle at L4. We then determined the association between overall mortality and the muscle size and muscle attenuation, while adjusting for demographic variables (age, sex, ethnicity, and body mass index), American Society of Anesthesiologists (ASA) classification, and Charlson comorbidity index (CCI).
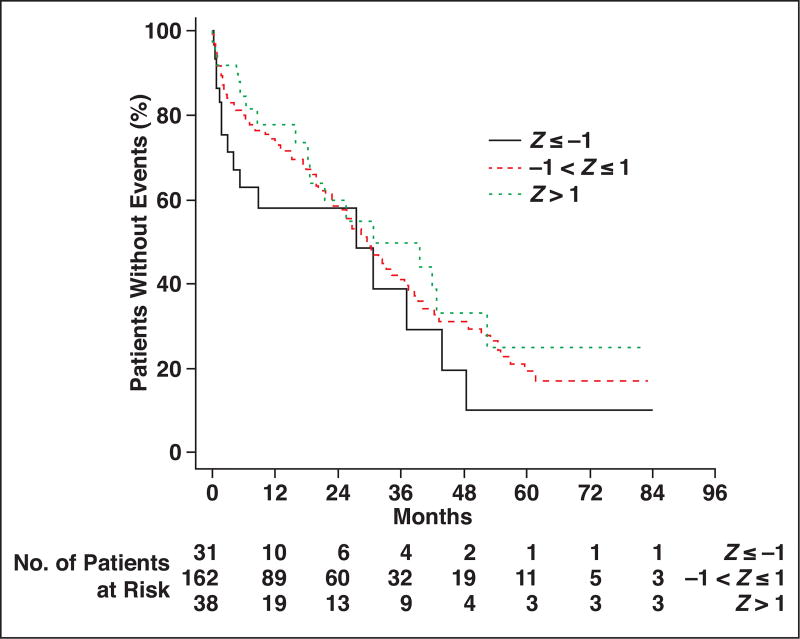
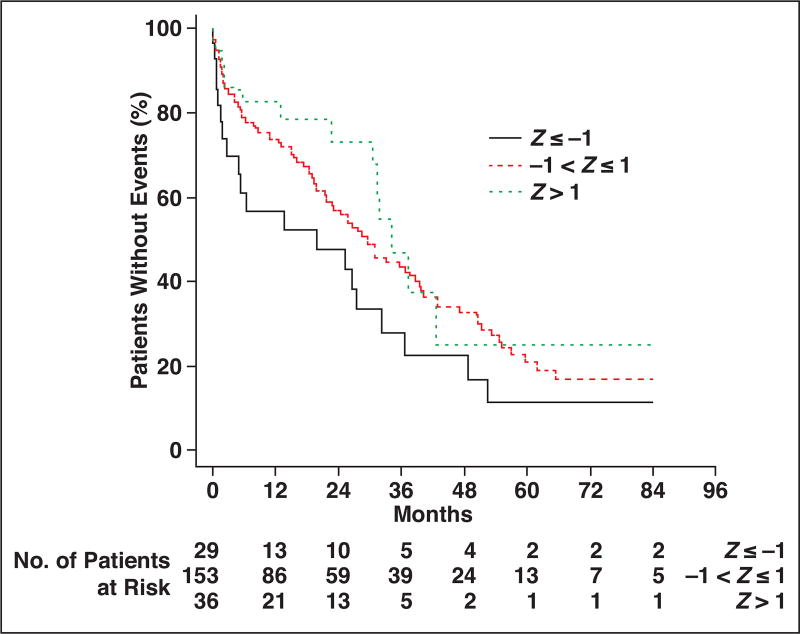
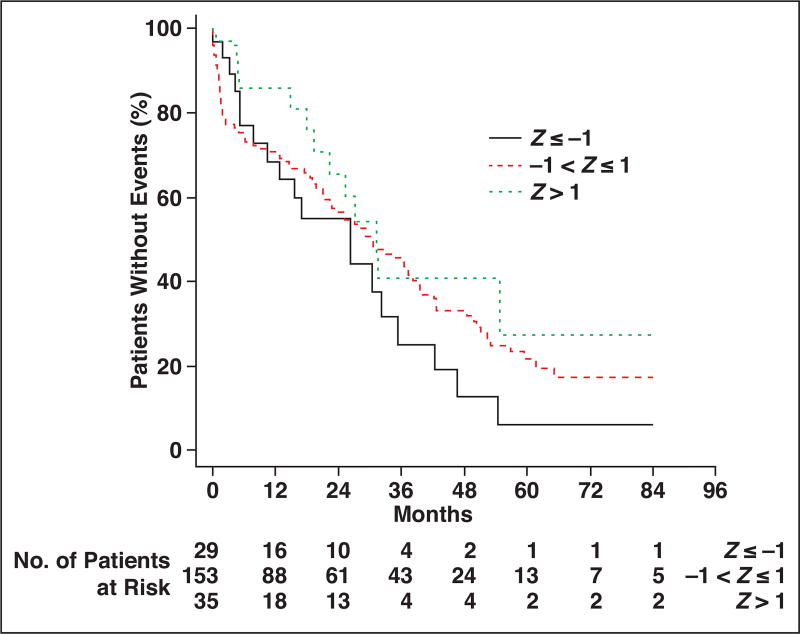
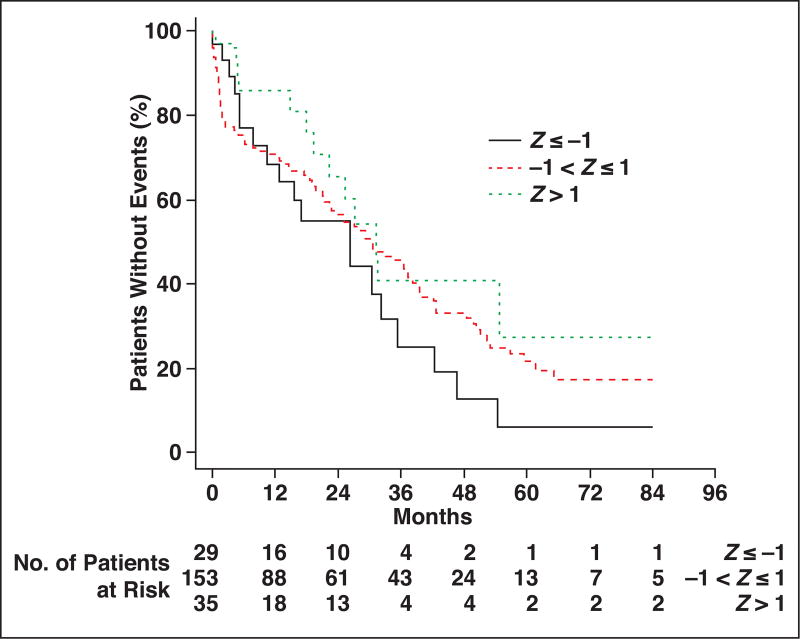
The overall mortality rate increased from 28.3% at 1 year to 79.5% at 5 years. Mortality was associated with decreased thoracic muscle size (odds ratio [OR], 0.66; 95% CI, 0.49-0.87). This association persisted after adjusting for demographic variables (OR, 0.69; 95% CI, 0.50-0.95), the ASA classification (OR, 0.70; CI, 0.51-0.97), and the CCI (OR, 0.72; 95% CI, 0.52-1.00). Similarly, decreased survival was associated with decreased thoracic muscle attenuation after adjusting for all of these combinations of covariates (OR, 0.67-0.72; 95% CI, 0.49-0.99). Decreased lumbar muscle size and attenuation trended with decreased survival but did not reach statistical significance.
In older adults with hip fractures, CT findings of decreased thoracic paravertebral muscle size and attenuation are associated with decreased overall survival.
我们的目的是确定在常规CT扫描中测量的肌肉横截面积和衰减与老年髋部骨折患者死亡率之间的关联。
对髋部骨折患者进行了一项为期10年的回顾性研究,纳入标准如下:年龄65岁及以上,首次接受手术治疗的髋部骨折,以及胸部、腹部或骨盆的CT扫描。共纳入274例患者(70.4%为女性;平均[±标准差]年龄为81.3±8.3岁)。在每次CT扫描中,两名阅片者独立测量T12椎体旁肌肉和L4腰大肌的大小(横截面积,根据患者身高进行指数化)和衰减。然后,我们在调整人口统计学变量(年龄、性别、种族和体重指数)、美国麻醉医师协会(ASA)分级和Charlson合并症指数(CCI)的同时,确定总死亡率与肌肉大小和肌肉衰减之间的关联。
总死亡率从1年时的28.3%上升至5年时的79.5%。死亡率与胸肌大小减小相关(比值比[OR]为0.66;95%可信区间[CI]为0.49-0.87)。在调整人口统计学变量(OR为0.69;95%CI为0.50-0.95)、ASA分级(OR为0.70;CI为0.51-0.97)和CCI(OR为0.72;95%CI为0.52-1.00)后,这种关联仍然存在。同样,在调整所有这些协变量组合后,生存率降低与胸肌衰减降低相关(OR为0.67-0.72;95%CI为0.49-0.99)。腰大肌大小和衰减降低与生存率降低呈趋势相关,但未达到统计学显著性。
在老年髋部骨折患者中,CT显示胸段椎体旁肌肉大小和衰减降低与总生存率降低相关。