Althunian Turki A, de Boer Anthonius, Klungel Olaf H, Insani Widya N, Groenwold Rolf H H
Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute of Pharmaceutical Sciences, Utrecht University, PO Box 80082, 3408 TB, Utrecht, The Netherlands.
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Huispost Str. 6.131, 3508 GA, Utrecht, The Netherlands.
Trials. 2017 Mar 7;18(1):107. doi: 10.1186/s13063-017-1859-x.
There is no consensus on the preferred method for defining the non-inferiority margin in non-inferiority trials, and previous studies showed that the rationale for its choice is often not reported. This study investigated how the non-inferiority margin is defined in the published literature, and whether its reporting has changed over time.
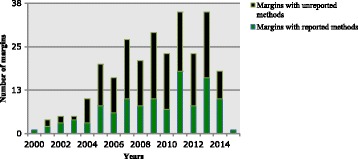
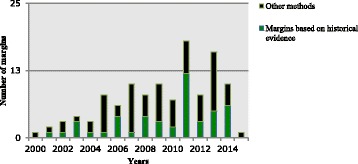
A systematic PubMed search was conducted for all published randomized, double-blind, non-inferiority trials from January 1, 1966, to February 6, 2015. The primary outcome was the number of margins that were defined by methods other than the historical evidence of the active comparator. This was evaluated for a time trend. We also assessed the under-reporting of the methods of defining the margin as a secondary outcome, and whether this changed over time. Both outcomes were analyzed using a Poisson log-linear model. Predictors for better reporting of the methods, and the use of the fixed-margin method (one of the historical evidence methods) were also analyzed using logistic regression.
Two hundred seventy-three articles were included, which account for 273 non-inferiority margins. There was no statistically significant difference in the number of margins that were defined by other methods compared to those defined based on the historical evidence (ratio 2.17, 95% CI 0.86 to 5.82, p = 0.11), and this did not change over time. The number of margins for which methods were unreported was similar to those with reported methods (ratio 1.35, 95% CI 0.76 to 2.43, p = 0.31), with no change over time. The method of defining the margin was less often reported in journals with low-impact factors compared to journals with high-impact factors (OR 0.20; 95% CI 0.10 to 0.37, p < 0.0001). The publication of the FDA draft guidance in 2010 was associated with increased reporting of the fixed-margin method (after versus before 2010) (OR 3.54; 95% CI 1.12 to 13.35, p = 0.04).
Non-inferiority margins are not commonly defined based on the historical evidence of the active comparator, and they are poorly reported. Authors, reviewers, and editors need to take notice of reporting this critical information to allow for better judgment of non-inferiority trials.
在非劣效性试验中,对于定义非劣效性界值的首选方法尚无共识,并且先前的研究表明,选择该界值的理由通常未被报道。本研究调查了已发表文献中如何定义非劣效性界值,以及其报告情况是否随时间而变化。
对1966年1月1日至2015年2月6日期间发表的所有随机、双盲、非劣效性试验进行了系统的PubMed检索。主要结局是由活性对照的历史证据以外的方法定义的界值数量。对此进行了时间趋势评估。我们还将定义界值方法的报告不足作为次要结局进行评估,以及这是否随时间而变化。两个结局均使用泊松对数线性模型进行分析。还使用逻辑回归分析了定义方法报告较好的预测因素以及固定界值方法(历史证据方法之一)的使用情况。
纳入了273篇文章,其代表273个非劣效性界值。与基于历史证据定义的界值相比,由其他方法定义的界值数量无统计学显著差异(比值2.17,95%置信区间0.86至5.82,p = 0.11),且这并未随时间而变化。未报告方法的界值数量与报告了方法的界值数量相似(比值1.35,95%置信区间0.76至2.43,p = 0.31),也未随时间而变化。与高影响因子期刊相比,低影响因子期刊中定义界值的方法报告较少(比值比0.20;95%置信区间0.10至0.37,p < 0.0001)。2010年美国食品药品监督管理局(FDA)指南草案的发布与固定界值方法报告的增加相关(2010年之后与之前相比)(比值比3.54;95%置信区间1.12至13.35,p = 0.04)。
非劣效性界值通常并非基于活性对照的历史证据来定义,且报告情况不佳。作者、审稿人和编辑需要注意报告这一关键信息,以便对非劣效性试验进行更好的判断。